Playlist
Show Playlist
Hide Playlist
Diagnoses of Reproductive Syndromes & Deficiencies


-
Slides Reproductive Pathology Differential Diagnoses.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
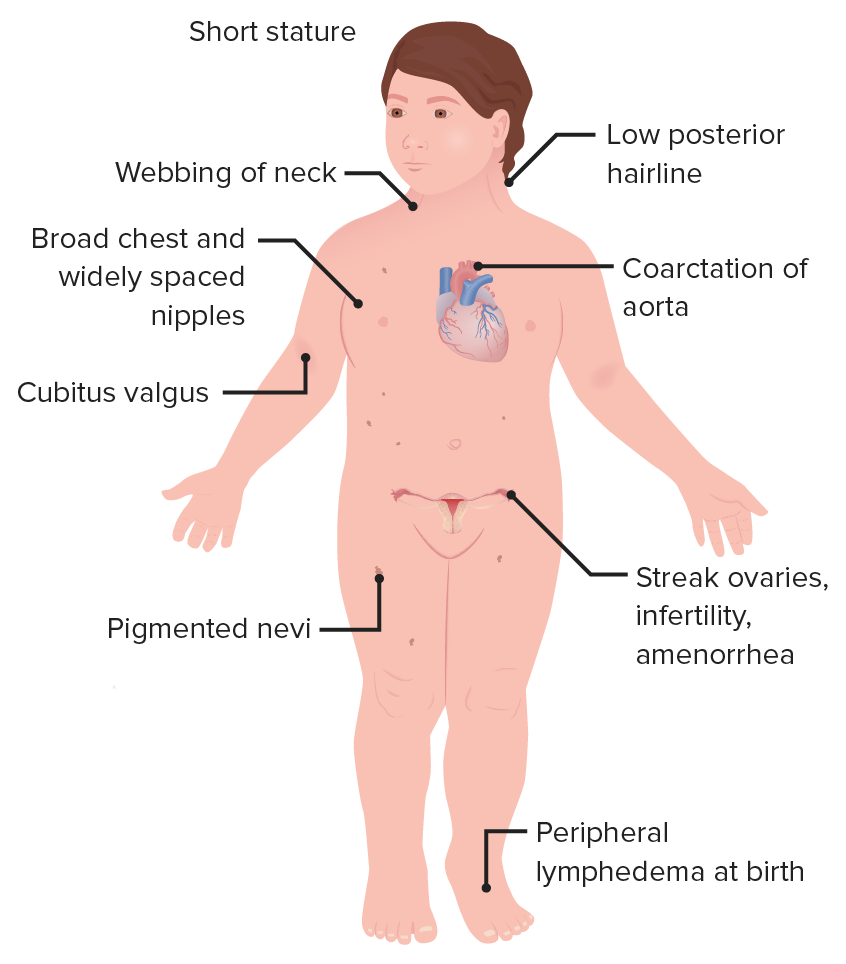
00:00 In this section, we’ll take a look at reproductive pathology differential diagnoses. You have just been waiting to get to this section so that you’re able to identify your patients. So without further ado, let’s begin. Differential diagnoses. Well, these are common conditions that students doctors, residents, anyone in the medical field wishes to make sure that they have firmly implanted in their head. Let’s begin. The conditions include Turner syndrome. Quickly think to yourself as to what may then your patient look like. She has webbing of the neck. 00:33 She came in with primary amenorrhea or maybe the mother brought her in with primary amenorrhea at the age of 16 or lack of menses. She might have increased blood pressure in upper extremity and lower blood pressure in the lower extremity, coarctation of aorta. 00:48 Maybe she has a crescendo-decrescendo type of systolic murmur that is heard best at the second right intercostal space, aortic stenosis. Turner, YY male, XYY. More common than one would think. 1 in 1000. Look for a patient who might be in the armed forces, maybe marine. 01:09 Meaning to say, these individuals are highly recruited by the armed forces because they have an extra Y chromosome which then provides them with interesting characteristics. 01:20 I’m being stereotypical here but on purpose, so that you’d be able to quickly identify your patient. Remember placental aromatase deficiency. Remember what aromatase does? It takes the testosterone and converts it into your estrogen. What may then happen if fetus is not able to properly do that? Then 5?-reductase deficiency. These are enzyme deficiencies that once again people get confused with but you no longer will. Kallmann syndrome, in Kallmann syndrome, you begin way up in the hypothalamus in which with your gonadotropic access, you don’t have enough GnRH. What else is this patient not exhibiting? He or she is unable to properly smell. So, exhibiting the inability to smell, in other words, anosmia. Let us now dive specifically into Turner syndrome and begin by talking about why the ovaries aren’t working. Remember in Turner syndrome that there is a condition or there is a description called streak ovaries. The streak ovaries refer to the fact that the ovaries are dysfunctional. The type of dysfunction you would then diagnose this as would be a dysgerminoma. Your next order of business would be, well if the ovaries aren’t working properly then what kind of hypogonadism would this be? Primary hypogonadism. If the ovaries aren’t working properly then you do not have or she does not have enough estrogen. She’s going to present with amenorrhea even at the age of 14 and 15, primary. If there is no estrogen, there is going to be an increase in gonadotropins, thus, you would call this primary hypogonadism, hypergonadotropic hypogonadism. All this we've reviewed and up until this point, it should make perfect sense. Let’s take a look at YY syndrome, underdiagnosed. 03:19 So the fact that you find this to be 1 in 1000, which seems to be quite common as is might actually be more common in our society. It’s noninherited condition. Phenotypically, you're going to have a male. Phenotypically, you have a male. Genotypically, take a look, XYY. 03:37 That’s a lot of Y activity. Therefore look for a male who is quite tall, quite masculine, and perhaps doesn’t even have much of a conscience. So therefore, you can see as to how perhaps, this individual might join the armed forces because that aggressive behavior that this male is exhibiting lands himself perfectly to armed forces. Interesting. Placental aromatase deficiency, remember this enzyme? Unable to properly convert your testosterone. 04:12 into estrogen. So therefore, this fetus is going to have increased testosterone activity. 04:19 5?-reductase deficiency, this is a genetic issue. If the enzyme is not even present, then you’re not able to properly convert your testosterone into DHT. Stop there for a second. 04:34 Make sure that you’re completely comfortable with the normal activity of the enzyme aromatase with 5?-reductase. Both of these are responsible for important conversion. 04:45 I’ll give you the symptoms of a patient which I haven’t given you here but I will give it to you coming up. In Kallmann syndrome, I’ve told you at this point, your best thing to do here is for you to memorize that you do have problems with the hypothalamus, in which the patient is not releasing GnRH. Therefore, you would call this tertiary, technically tertiary type of hypogonadism. You would call this hypogonadotropic hypogonadism. What else did I say about this patient? I’ve mentioned that a few times now? That your patient is not able to properly smell, anosmia. Let’s talk about symptoms further about the same conditions from the previous discussion. With Turner syndrome, a short stature if left untreated. 05:35 If you’re thinking about YY random nondisjunction event, paternal meiosis phase 2, placental aromatase activity is lost. So therefore, there’s going to be increased testosterone as you had correctly pointed out, masculinization. And if it’s a female, she has ambiguous genitalia. What does that even mean? What’s the most important sign as you being a clinician are going to then exhibit or find or detect in a young infant girl? Clitorimegaly, the clitoris looks like a penis, ambiguous genitalia because of all that testosterone activity. 5?-reductase deficiency, this goes back to making sure that you understand your physiology. Genotypically, you’re male affected only because why? Because males require testosterone to be converted into DHT. Can it protect us from going to happen. The testosterone is present but the DHT is not. Therefore, what kind of male sexual structures will then be affected, internal of external male structures? DHT gives rise to external. That’s a possibility. I want you to focus upon the genotype of both your aromatase and your 5?-reductase. Most commonly, placental aromatase deficiency, you’re looking for a female 46 XX genotypically, she has too much testosterone activity. Look for that presentation, most commonly. 5?-reductase deficiency, this patient has to be a male. Remember, a female doesn’t require large amounts of testosterone. 07:20 So look for only male, 46 XY genotypically. With Kallmann syndrome, because your patient doesn’t have enough GnRH, that means failure to complete puberty due to the defective migration. And your patient once again is not able to smell. Let’s continue further with a little bit of details for each, each of the diagnosis. Hope you’re having a good time now identifying your patient. You should have fun with this. Now with Turner syndrome, we talked about the streak ovaries. This is then referred to as being a dysgerminoma. What is this then equivalent to in a male? The germ cell tumor known as your seminoma, YY, maybe associated with severe acne vulgaris, lots of masculinization taking place. Aromatase, lots of testosterone and androstenedione. Remember that female and this young girl may present with ambiguous genitalia. 5?-reductase deficiency, inability to convert your testosterone into DHT. Kallmann syndrome, finally, you see it here in words, the official verbiage of anosmia. Which means what? Inability to smell. You must know that there’s not only was there failure of migration of the cells required to produce GnRH but there's failure of migration of the cells into the olfactory bulb resulting in anosmia. 08:44 I specifically went through this pattern of recognition and description because I want you to keep being able to compare these cases and these patients and be able to identify clearly how you can distinguish one patient from the other. So by the time you take your boards and you’re in your wards, my goodness, it will be so easy for you as a clinician to identify your patient and there you go. Success is yours. More details about Turner. 09:15 Remember the cystic hygroma? Cystic hygroma, you must know the other name for it. 09:21 Not the webbing, the webbing is a “layman term.” But the cystic hygroma is really a lymphangioma. Do you see as to how I emphasized the lymph? This is not a hemangioma nor is it a leptomeningeal. This is a lymphangioma, cavernous in the back of the neck. 09:41 So what are you going to find? Lymphedema. Not only could you find lymphedema in the back of the neck. 09:47 In fact, you might even detect this on ultrasound in a pregnant woman. So she is carrying a fetus unfortunately who is destined to have Turner syndrome. You take a look at the back of the neck in ultrasound, you’re going to find fluid accumulating. It’s that clear. But not only would you find lymphedema there, you could also find it in the feet and hands. Keep that in mind. 10:11 In YY, autism spectrum, learning disability and quite aggressive. Be careful to use this as a differential for autism. Genotypically XYY. Presents with maternal virilization during pregnancy. 10:26 That’s important. It presents with maternal virilization. What do you know about this enzyme? If it’s not present, placental aromatase deficiency. What happens is the fact that the fetal androgens that were supposed to return to estrogen are not. They will cross the placenta. 10:43 The pregnant woman is showing signs of virilization. What does that mean? That the mother might actually start developing acne. Big time pay attention to that. 5?-reductase deficiency, here, ambiguous genitalia. Why? Well, if there is going to be decreased DHT, you might not be able to properly form that penis. So what’s my genotype in 5?-reductase deficiency? Do you see as to how it’s important. I really want you to get in the habit of differentiating geno and pheno, geno and pheno. Genotypically, 5?-reductase deficiency has to be a male. 11:24 So if you’re seeing ambiguous genitalia, the male penis may look like a clitoris or clitorimegaly. 11:31 Is that clear? Whereas, if it was placental aromatase deficiency, most likely genotypically was a female, XX. So when we say ambiguous genitalia in that young girl, we’re referring to clitorimegaly. The clitoris looks like a penis. Make sure you spend a second there and be able to identify the description of ambiguous genitalia either in a boy or in a girl and what that means in terms of the embryologic pathogenesis. Kallmann syndrome, low sperm count results in infertility. Why? Can you put it altogether now? The decreased GnRH, no LH and FSH, definitely no testosterone or decreased testosterone. That decreased testosterone does not allow for proper sperm maturation. Turner syndrome, let me give you more symptoms. 12:24 At this point, it should be so obvious. Your patient has Turner. The rest of this will behave the same way. Remember the aortic valve. Close your eyes, aortic valve. How many cusps? One, two, three. Every single valve in the heart has three cusps except the mitral, bicuspid, right? What if you have a patient who has bicuspid aortic valve? This is a congenital issue. 12:49 Is Turner a congenital disease? Of course it is. So now you have a patient who has developed congenital bicuspid aortic valve. How does that manifest? Good, aortic stenosis. Could it be aortic regurg? It could. It could. We had that discussion earlier in cardiology. But for most common at this point, think of bicuspid aortic valve then therefore causing aortic stenosis. 13:17 Think about that patient, young, maybe 30s, maybe even younger. You hear a crescendo-decrescendo murmur. Where? Second intercostal right space and the murmur is going to radiate up into carotid. What about the kidney? The inferior pole most likely, inferior pole with the kidney in a fetus gets fused and during the migration may then get cut with the inferior mesenteric artery. We’re talking about horseshoe kidney. I want you to jump over to 5?-reductase deficiency. There is going to be increased growth of external genitalia. 13:54 Why? What ends up happening here is the fact that at some point during puberty, pay attention, during puberty is when all of a sudden, there’s going to be testosterone activity. 14:07 That testosterone activity in this patient, it’s quite peculiar. So you pay attention to this. 14:13 All of a sudden, there’s going to be increased growth of external genitalia. Why did this not occur during fetal life? Because there is 5?-reductase deficiency. There wasn’t enough DHT, dihydrotestosterone. Take a look at the previous statement of ambiguous genital. That was in a new born, just about, an infant, a boy, a baby boy. The penis was really tiny. 14:35 Then during puberty, remember the patient still has testosterone, the body will find a way to increase the size of the penis. The external genitalia will increase in size during puberty. 14:48 Look for that description please for 5?-reductase deficiency. Notice, you don’t find that anywhere else with any other patients here. In Kallmann syndrome, if the female, she’s not going to have menses. I'm going to name amenorrhea, anosmia, hypogonadotropic hypogonadism. Spend a little bit of time. You go through every single one of these diseases. 15:10 You go through exactly what I’ve done. You need to go through this column by column or row by row or whatever it is. Make sure that you’ll clearly be able to walk through your labs, your patient, and how they’re presenting. You’ll be in fantastic shape. Turner syndrome, what do you want to do here? Well, next step is management. I’m not going to every single management. Question is not asked but the common questions for Turner syndrome: exogenous estradiol, progesterone administered for possible conception. Remember, your patient here has what kind of issue? Primary hypogonadism. So why not try to replace the estrogen and progesterone that’s missing? By doing so, you might actually facilitate pregnancy. Fantastic news. 5?-reductase deficiency management. Testosterone and estrogen levels are normal. In labs with Kallmann syndrome, pretty much everything is decreased because your problem begins with the GnRH. LH normal or perhpas even increased in 5?-reductase deficiency. The internal genitalia are normal. Big time difference as a differential. I’ll talk to you about this in great detail. Androgen insensitivity syndrome. 16:30 In androgen insensitivity syndrome, do you remember that patient? Genotypically male. What about this patient 5?-reductase deficiency? Genotypically male. You do a pelvic exam on an androgen insensitivity syndrome, a pelvic exam. What? You told me he’s genotypically male. Correct. 16:50 But the male has a vagina. When you do a pelvic exam, it’s a blind pouch. That's androgen insensitivity syndrome. In 5?-reductase deficiency, tell me about the testosterone. No problems there. The testosterone will give rise to internal genitalia. These become important big time.
About the Lecture
The lecture Diagnoses of Reproductive Syndromes & Deficiencies by Carlo Raj, MD is from the course Reproductive Hormone Disorders.
Included Quiz Questions
Which of the following is NOT seen in Turner syndrome?
- Hypogonadotropic hypogonadism
- Cystic hygroma
- Gonadal streaks
- Coarctation of the aorta
- Mosaic 46 XX/45 XO
Which of the following is NOT a characteristic of a double Y male?
- Autosomal recessive status
- XYY
- Tallness
- Aggressiveness
- Having a pattern seen in 1:1,000
Which combination is INCORRECT?
- 5-alpha-reductase deficiency — high DHT
- Kallmann syndrome — anosmia
- Kallmann syndrome — hypogonadotropic hypogonadism
- 5-alpha-reductase deficiency — autosomal recessive
- Placental aromatase deficiency — low estrogen levels
Which combination is INCORRECT?
- 5-alpha-reductase deficiency — low testosterone
- Turner syndrome — short stature
- Double Y male — non-disjunction event
- Placental aromatase deficiency — female XX
- Kallmann syndrome — delayed puberty
Which condition is associated with a high testosterone level?
- Placental aromatase deficiency
- Kallmann syndrome
- Turner syndrome
- Hypogonadotropic hypogonadism
Which condition is NOT paired correctly with a finding?
- Turner syndrome — tricuspid aortic valve
- Turner syndrome — horseshoe kidney
- Double Y male — autism
- Kallmann syndrome — infertility
- 5-alpha-reductase deficiency — ambiguous genitalia
Which of the following conditions might be treated with estradiol 17B?
- Turner syndrome infertility
- Masculinization
- Autism in a double Y male
- 5-alpha-reductase deficiency
- Lymphedema in Turner syndrome
Author of lecture Diagnoses of Reproductive Syndromes & Deficiencies

Carlo Raj, MD
Customer reviews
3,7 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
I love Dr. Raj's lectures. He makes complex topics easier to understand and remember.
Shouldn't be popping back and forth between disorders- makes for very jumbled learning. Should talk through this disease in full then move on.
clear and concise. provides a great sieve for distinguishing between the different sex development disorders.
