Playlist
Show Playlist
Hide Playlist
Diabetic Glomerulosclerosis and Renal Amyloidosis


-
Slides MembranoproliferativeGlomerulonephritis RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
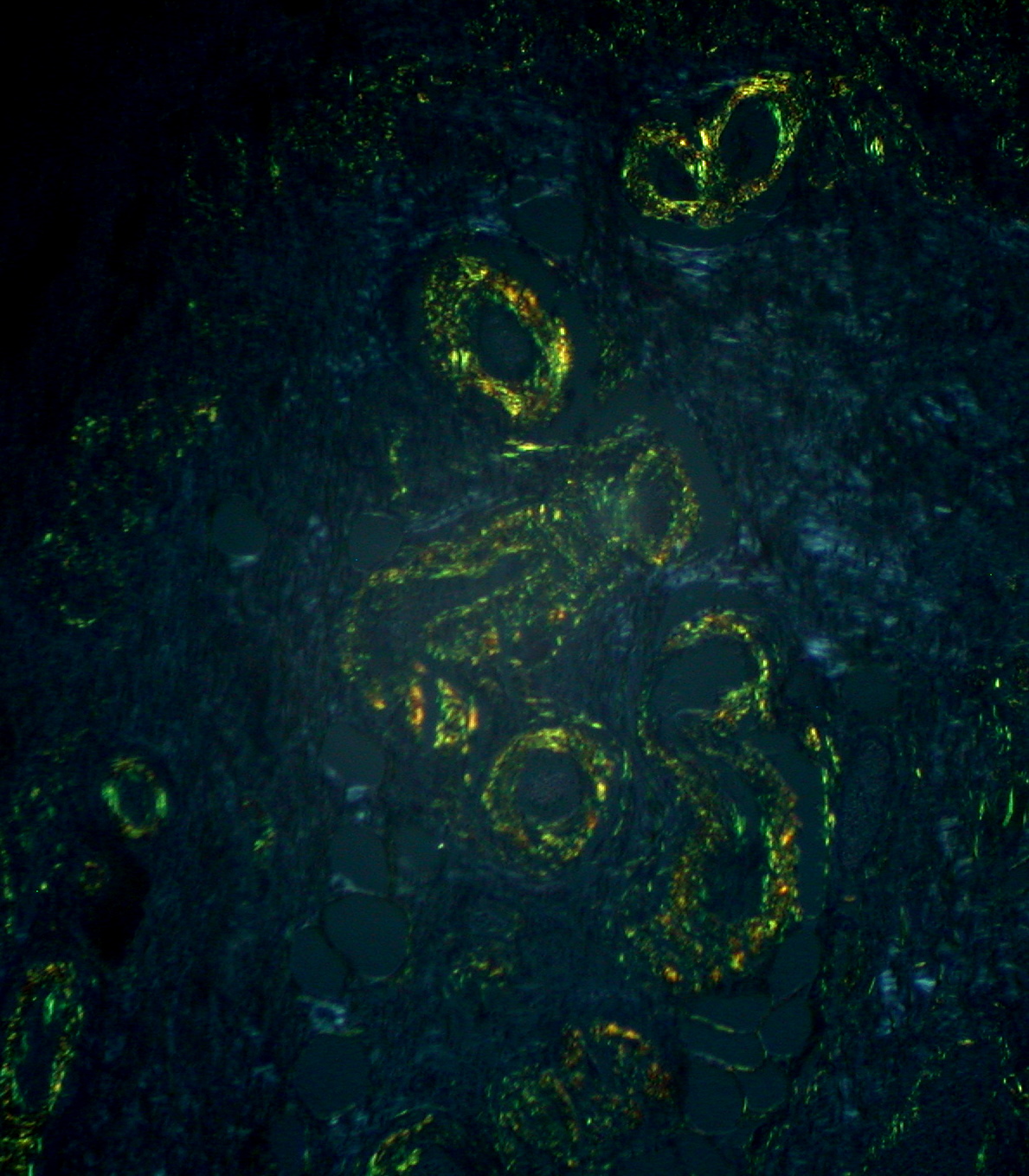
00:00 What you're seeing here on light microscopy is in fact that nodule, but it took a long time for you to develop and hence, what we did earlier, we walked up and down the body. 00:09 Meaning to say, diabetic microangiopathy, retinopathy, talked about cataracts. 00:14 I gave you two different types of pathways for damage, including non-enzymatic glycosylation, hyaline arteriolosclerosis, and blood vessels are affected. 00:24 Now, the picture or the arrow on the right represents hyaline arteriolosclerosis. 00:32 So that is a blood vessel. Do you understand that? And that black head, by looking at that you can't tell if it’s afferent or efferent. 00:40 But what’s the first arteriole to be affected? The efferent. What's that called? When you have massive efferent arteriolosclerosis, what does it do to the glomerulus? The spanking. What's that called? Hyperfiltration disease. 00:55 Increase in proteinaceous material in the wall of the vessel. 00:59 Next, that nodule that you're seeing is deposition of your type IV collagen, here, this would be in the mesangium. 01:07 Where else could it be? Well, you could also have deposition in different parts of your kidney. 01:12 At this point, we have completed the discussion on diabetic nephropathy in great detail. 01:17 We’re gonna continue through systemic disease. 01:20 And at this point, ladies and gentlemen, we’ll take a look at what's known as renal amyloid. 01:25 What does that mean? Well, I want you to take a look at the pictures on your right. 01:29 Top and bottom, congo red stain. 01:32 What does that mean? Amyloid. 01:35 Amyloid means what to you on congo red stain? Apple-green birefringence, is that clear? So what kind of issue you might be thinking about? High on your differential. 01:44 How about Bence Jones proteins? What does that mean to you? Bence Jones protein represents your light chains, kappa/lambda, kappa moreso. 01:53 In other words, you're looking at immunoglobulins depositing. 01:58 Chronic inflammation, rheumatoid arthritis, plasma cell disease such as multi-myeloma. 02:05 In the amyloid here, is the fact that it’s depositing congo red stain. 02:10 Dangerous? Yeah. 02:11 As soon as you start amyloid depositing on organs, oftentimes, the only-your next step in management is organ transplant. 02:19 Renal amyloid associated with secondary amyloidosis. That is important. 02:24 If there is amyloidosis, congo red stain, we talked about how this stain appears of being apple-green birefringence. 02:31 If that is on H&E, that would be a bit more difficult. 02:34 This kinda looks like maybe a global proliferation and looks rather eosinophilic and it pretty much affects the entire glomerulus. 02:43 Now, this is a little bit more difficult for you to follow but if your patient has lytic bone lesions, you end up finding increase in IgG in a bone marrow aspirate, you’ll find these plasma cells. 02:54 Then this has to be amyloid and your next step in management? Congo red stain to find that apple-green birefringence. 03:00 But there is a difference in terms of how it appears on H&E versus how it does on congo red stain.
About the Lecture
The lecture Diabetic Glomerulosclerosis and Renal Amyloidosis by Carlo Raj, MD is from the course Glomerulonephritis.
Included Quiz Questions
Which of the following is NOT associated with any potential etiologies for renal amyloidosis?
- Nephritic factor
- Rheumatoid factor
- IgM monoclonal protein
- Plasma cell dyscrasias
- Bence Jones proteins
What is the special stain required to confirm the presence of amyloidosis?
- Congo red stain
- Hematoxylin and eosin stain
- Prussian blue stain
- Mucicarmine stain
- Periodic acid-schiff stain
What would you see with H&E stain of a biopsy specimen with renal amyloidosis?
- Eosinophilic acellular material in glomerular tuft and capillary walls.
- Proliferation of parietal epithelial cells occupying Bowman’s capsule
- Diffuse thickening of glomerular basement membrane
- Empty vacuoles in the glomeruli
- Normal glomeruli
Which of the following is a typical appearance of Amyloidosis on a Congo red stain under polarized light?
- Apple-green birefringence
- Blue-violet birefringence
- Deep brown birefringence
- Deep reddish-purple appearance
- Dark grey to black appearance
Which of the following is associated with potential etiologies of renal amyloidosis?
- Bence Jones proteins
- Nephritic factor
- C3 convertase
- Uric acid
- Hypercalcemia
Author of lecture Diabetic Glomerulosclerosis and Renal Amyloidosis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
