Playlist
Show Playlist
Hide Playlist
Clinical Anatomy of Breast Cancer

-
Slides Breast Female Repro.pdf
-
Download Lecture Overview
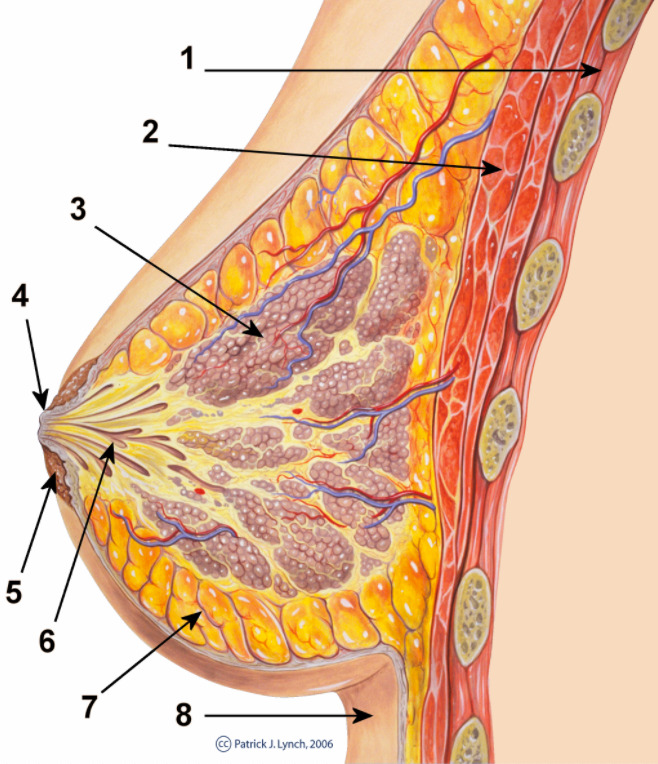
00:01 I told you earlier that I would walk you through the clinical anatomy of breast cancer. 00:05 On the left is your nipple and as you move from the nipple all the way down to stroma, we’ll take a look at various pathologies underneath. 00:14 With the nipple, two major issues that could occur. 00:17 You can have Paget’s disease or you could have acute mastitis. 00:22 Acute mastitis, you might have an abscess formation. 00:25 If there’s abscess formation, close your eyes, what does the breast look like in a female there? The center area might be a little bit yellowish and purulent and the surrounding tissue, inflammatory, will be erythematous. 00:37 Then you have Paget’s disease of the nipple. 00:39 And we’ll talk about that in greater detail. We have to. 00:41 This is mammary type, obviously. 00:44 From your nipple, you’ll then move into lactiferous sinus. 00:47 The major pathology that we discussed in lactiferous sinus thus far is intraductal papilloma. 00:54 Would you please take a look at how close your lactiferous sinus is to the nipple. 00:59 So therefore any lesion or pathology to the sinus is then going to result in -- 80% of your patient, what kind of discharge? Bloody or serous. 01:08 You could also have the mastitis that may affect this area as well, but superficially. Superficially. 01:14 After this, we’ll get into our ducts. 01:16 You have a big major and you have a little terminal duct. 01:20 Group them together, please. And you call them ductal. 01:24 In the previous discussion, we began with malignancy. 01:26 We looked at ductal carcinoma in situ. 01:29 That means that the ducts here, if they undergo cancerous change with maybe ductal hyperplasia and specifically I told you about comedocarcinoma that the basement membrane is going to be intact. 01:42 But that’s where you’d find your ductal carcinoma in situ. 01:45 And then if you finally go distally, you see these lobules? There down distal, down by the stroma or back deep by the stroma. 01:54 And then we’ll talk about lobular carcinoma in situ and invasive lobular cancer. 02:01 What’s then hanging on to the breast? Or should I say the breast is then implanted onto the stroma. 02:08 So think of this as being kind of like your scaffolding. 02:11 The stroma here, a couple of important benign tumors that we have discussed. 02:17 Fibroadenoma, how old is your patient? Young, estrogen-responsive, and with fibroadenoma, you’re thinking about fibrous change. 02:28 Is it small or big, fibroadenoma? A small tumor. 02:33 Phyllodes tumor. 02:35 Age range? Elderly, postmenopausal. Commonly sixth decade. 02:40 In terms of the size of the tumor, small or large? Large. 02:44 What about it’s increased risk of cancer? Much greater than fibroadenoma. 02:50 I asked you kindly to make sure that you compare and contrast phyllodes and fibroadenoma. 02:54 I’ve just given you brief little points. 02:56 Let’s continue, please. 02:58 Spend a little bit time make sure that you’re completely comfortable up and down the breast apparatus.
About the Lecture
The lecture Clinical Anatomy of Breast Cancer by Carlo Raj, MD is from the course Reproductive Pathology: Breast Disease with Carlo Raj.
Included Quiz Questions
Which of the following conditions does NOT involve the nipple?
- Fibroadenoma
- Acute mastitis
- Ductal ectasia
- Intraductal papilloma
- Paget disease of the breast
Which of the following conditions of the breast is MOST likely to present with a yellowish or purulent discharge from the nipple with erythema of the surrounding tissue?
- Acute mastitis
- Fibroadenoma
- Phyllodes tumor
- Comedocarcinoma
- Intraductal papilloma
Author of lecture Clinical Anatomy of Breast Cancer

Carlo Raj, MD
Customer reviews
1,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
1 |
The professor seems to be too cold and the video could have way more images and interactions. I don't like this kind of video
