Playlist
Show Playlist
Hide Playlist
Cholecystitis: Diagnosis & Management

-
Slides Gallbladder.pdf
-
Download Lecture Overview
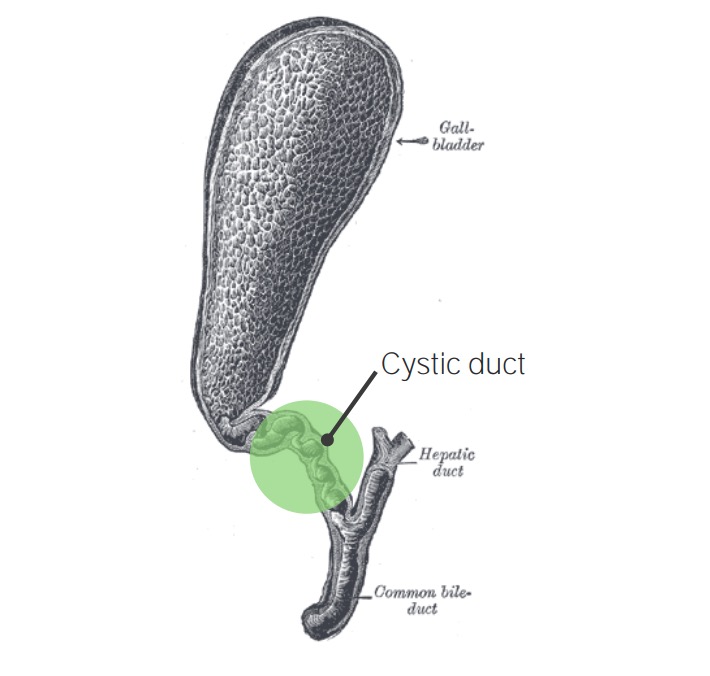
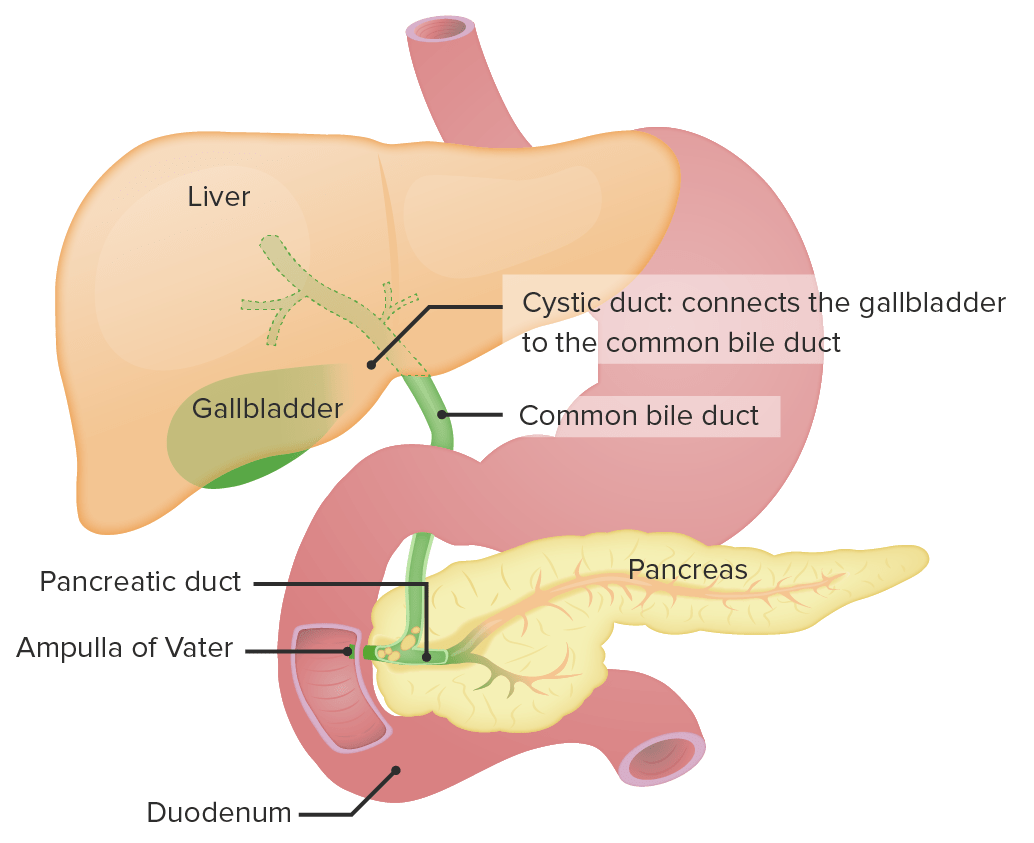
00:01 Diagnostic imaging is important in the diagnosis of cholecystitis. 00:05 An ultrasound has now become standard. Not only is ultrasound cheap, it doesn’t induce any radiation on the patient. 00:14 Nevertheless, it is operator-dependent. 00:16 In this image, you see a gallstone noted by the black arrow close to the neck of the gallbladder. Remember on ultrasound, fluid looks completely black. 00:28 In this ultrasound image, we see pericholecystic fluid. 00:32 See that stripe of black fluid between two thicken linings of the gallbladder Lastly, this is a demonstration of the wall thickening. 00:42 So remember on ultrasound, the classic threesome is wall thickening, pericholecystic of the wall thickening. 00:53 HIDA scan is also sometimes a useful adjunctive study. HIDA stands for hepatobiliary iminodiabetic acid. 01:02 And Hepatobiliary iminodiacetic acid is preferentially taken up by the liver and excreted. 01:12 By definition, acute cholecystitis is an obstruction of the cystic duct. 01:17 Therefore, after excretion of HIDA from the liver, there should be uptake in the gallbladder. 01:24 When there is no uptake in the gallbladder, it is suggestive of a complete obstruction of the cystic duct. 01:30 This is usually used as a confirmatory study if the ultrasound or physical findings are equivocal. 01:38 How do we manage gallstones? My decision tree involves whether or not the gallstone is associated with cholecystitis. 01:47 When associated with cholecystitis or infection of the gallbladder, typically antibiotics are given and surgery is recommended. 01:55 We usually offer surgery within 72 hours of the admission. 02:00 Without signs of cholecystitis but with abdominal pain, it is likely symptomatic cholelithiasis. 02:07 This disease does not require any antibiotics. Generally speaking, surgery can be performed on an elective basis. 02:14 In fact, many of these patients presenting to the emergency medicine have self-limited pain and are usually discharged and sent to a surgeon for outpatient referral. 02:26 Let’s pause for a moment. Are there any special considerations in pregnant women with acute cholecystitis? I’ll give you a minute to think about this. Remember, pregnant women have to undergo general anesthesia to undergo a laparoscopic cholecystitis. In general, during the first trimester, it is ill-advised to have a laparoscopic procedure performed under general anesthesia. If at all possible, we can temporize by treating the patient with antibiotics alone. Of course, if the mother’s life is in danger or is clinically deteriorating, then it’s most prudent to proceed with surgery. 03:06 Also remember, anatomically speaking, the uterus particularly the gravid uterus can be high up closer to the umbilicus. This makes entry for a laparoscopic procedure more hazardous. 03:20 Something to keep in mind when you’re offering surgery.
About the Lecture
The lecture Cholecystitis: Diagnosis & Management by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which of the following is the preferred choice for diagnosing acute cholecystitis if ultrasound imaging is equivocal?
- Hepatobiliary iminodiacetic acid (HIDA) scan
- CT imaging
- Endoscopic retrograde cholangiopancreatography
- Abdominal X-ray
- Surgical exploration
Which of the following is the best option for the management of acute cholecystitis?
- Antibiotics and urgent cholecystectomy
- IV fluids, antibiotics, pain control, and close observation
- Antibiotics and elective cholecystectomy
- Ursodeoxycholic acid and cholestyramine
- Endoscopic retrograde cholangiopancreatography
Author of lecture Cholecystitis: Diagnosis & Management

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
