Playlist
Show Playlist
Hide Playlist
Case: 67-year-old Woman with Headaches

-
Strowd CNS Tumors Pituitary Adenoma.pdf
-
Download Lecture Overview
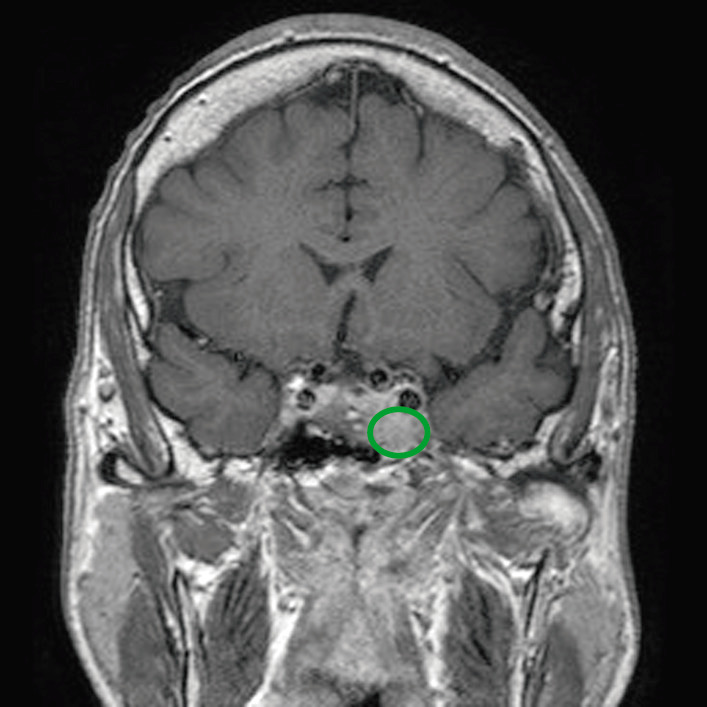
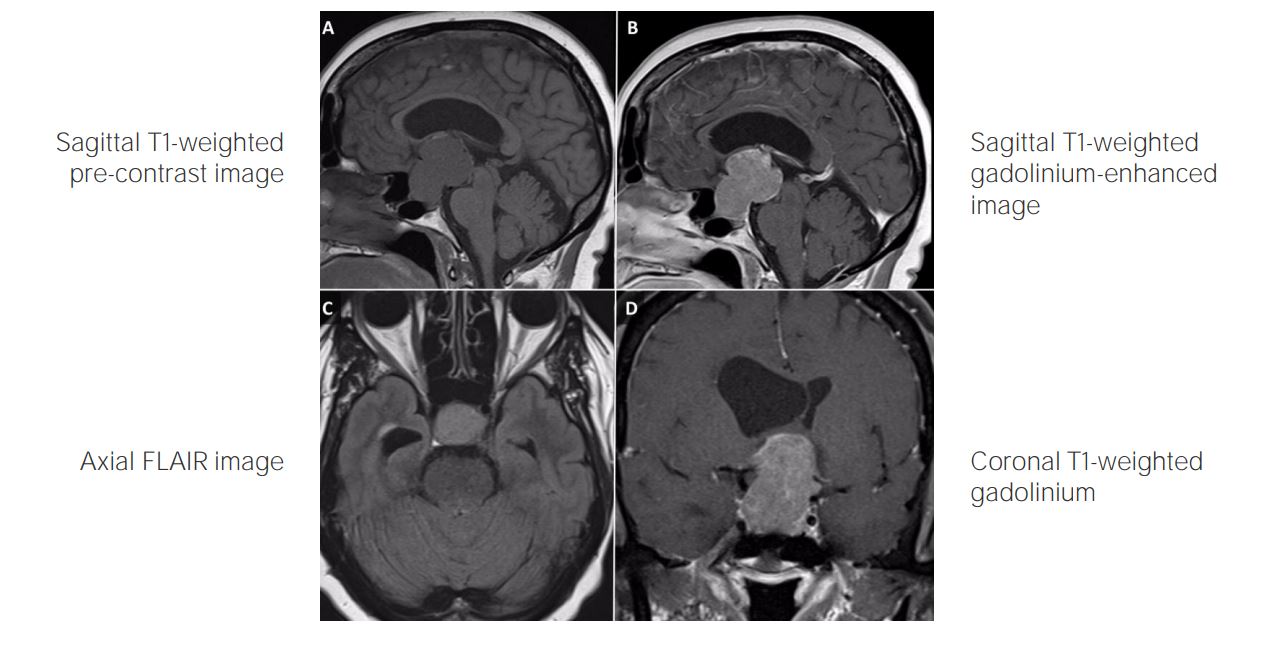
00:01 In this lecture, we're gonna talk about pituitary adenomas. 00:04 That third most common brain tumor, primary brain tumor, that arises in the midline structure of the sella turcica, the pituitary gland. 00:14 Let's start with a case. 00:16 This is a 67-year-old woman who presented with a 10-year history of chronic recurrent headaches that initially began after a motor vehicle accident. 00:25 In that accident, she suffered a nasal bone fracture, followed by repair and reconstruction of the nose. 00:32 A gadolinium-enhanced MRI showed an asymmetric enhancing mass within the right side of the sella turcica expanding into the cavernous sinus. 00:42 And that expanding indicates that this may be a tumor. 00:46 Laboratory workup, which is important for this patient was significant for a serum prolactin of 696, which is significantly elevated. 00:55 And we're going to learn that prolactin can be mildly elevated from tumors that impair and impede, and compress the pituitary stock or substantially elevated from tumors that generate prolactin secretion on their own. 01:10 The patient had normal serum cortisol, thyroid-stimulating hormone, free thyroxin, and insulin-like growth factor, other hormones made by the pituitary, and physiologically appropriate follicle-stimulating hormone or FSH, and luteinizing hormone or LH. 01:26 Ooh, big case. What's the diagnosis? Well, let's walk through this. 01:32 First of all, we see that the lesion is a lesion in the sella turcica. 01:36 And that expansion of this area suggests that this may be a tumor or a mass. 01:42 The laboratory evaluation for this patient is extremely important and we see a significantly elevated prolactin, and this is going to point us towards a prolactin secreting tumor, which is called a prolactinoma. 01:55 And we see that there's normal hormone function for the other pituitary hormones, things like cortisol, TSH, free T4, insulin-like growth factor, FSH, and LH. 02:07 This patient would undergo imaging. 02:09 And we read and heard about the MRI, and here you see that here. 02:13 This is a T1 image, a coronal T1 image, with gadolinium-enhancement with contrast. 02:19 And we can see the brain. 02:21 Beneath the brain in the midline is the optic chiasm. 02:25 And then we see this bone, this area of bone, that is the sella turcica, the seat, that the pituitary gland sits in. 02:32 In that area we see an enhancing mass, it's homogeneously enhancing, it's all white, and it's extending. 02:38 It appears to be extending out of the pituitary gland towards the cavernous sinus, which you can see here and the green arrows, and that extension out in the white arrow. 02:47 This is an asymmetric enhancing mass that appears to be arising from the pituitary stalker gland and extending along the dural surface. 02:56 So what's the diagnosis? Is this a brain metastasis, meningioma, pituitary adenoma, glioma, or vestibular schwannoma? Well, this doesn't seem like a vestibular schwannoma. 03:07 It's not in the right location. 03:08 And this is not the typical presentation, for of a patient with hearing loss. 03:12 Gliomas are uncommon outside of the brain or in the pituitary region. 03:17 And this looks more like something that is developing in a specific location, as opposed to in the brain parenchyma itself. 03:24 Brain metastasis can form in this location, but would often progress more rapidly than this patient who has a 10-year history of headaches suggesting a more slowly growing lesion. 03:35 Meningiomas can occur in that outer surface that outer covering of the brain, the meninges, but typically those develop from the meninges first, and grow into or over the pituitary and sella turcica as opposed to this lesion, which starts in the pituitary and grows out. 03:51 So this is our classic presentation of a pituitary adenoma. 03:54 This is a benign slow growing tumor that has been developing probably over the course of 10 years. 04:00 It sits within the sella turcica and is either impairing hormone function, or secreting hormone itself. 04:06 And for this patient, we would favor a prolactinoma. 04:12 How is this patient treated? Well, we'll get to treatment of pituitary tumors. 04:16 This patient was treated with a hormonal agent, cabergoline, which is a dopamine agonist. 04:22 She was treated 0.5 milligrams, two times per week. 04:25 And we see on this image dramatic reduction of that tumor over the course of one year. 04:30 And you can see that enhancing mass that was filling the sella turcica that was obstructing, and compressing the pituitary gland is now significantly smaller. 04:40 And we also would see improvement in this patient's prolactin level. 04:44 So substantial response to hormonal treatment which we'll talk about in the lecture.
About the Lecture
The lecture Case: 67-year-old Woman with Headaches by Roy Strowd, MD is from the course CNS Tumors.
Included Quiz Questions
A benign, slow-growing lesion in the sella turcica would suggest what diagnosis?
- Pituitary adenoma
- Pilocytic astrocytoma
- Meningioma
- Vestibular schwannoma
- Glioblastoma multiforme
Pituitary adenomas are associated with which of the following tumors?
- Prolactinomas
- VIPomas
- Medullary thryoid carcinomas
- Pheochromocytomas
- Zollinger–Ellison syndrome
Which of the following agents is the treatment of choice for prolactinomas?
- Cabergoline
- Cisplatin
- Cyclophosphamide
- Cytarabine
- Doxorubicin
Author of lecture Case: 67-year-old Woman with Headaches

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
