Playlist
Show Playlist
Hide Playlist
Carpal Tunnel Syndrome

-
Slides Carpal Tunnel Syndrome.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
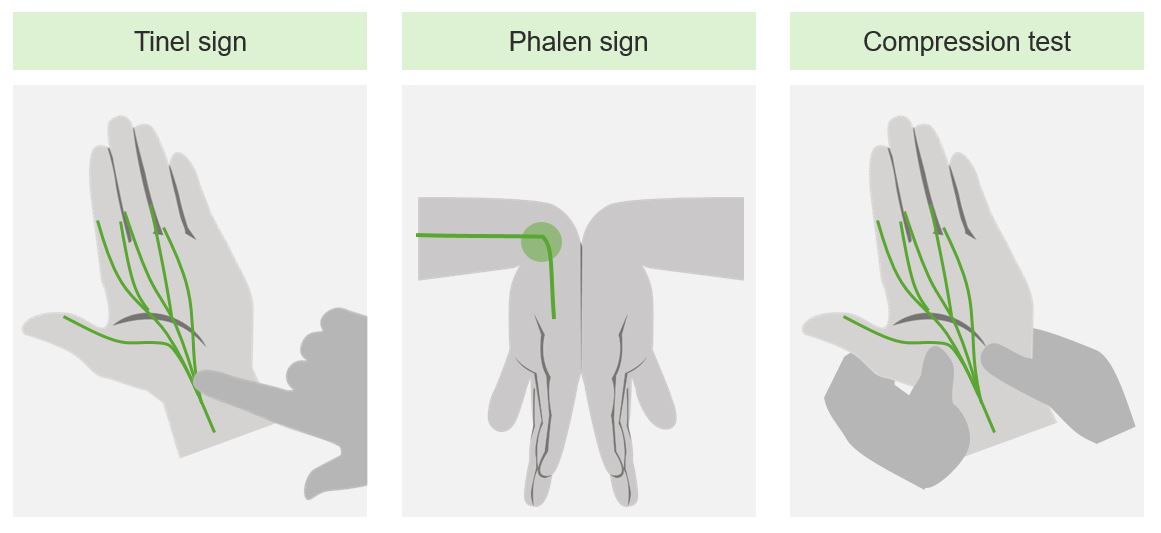
00:00 Carpal tunnel syndrome is a common condition that's very amenable to osteopathic manipulative medicine. 00:06 We’re going to talk about carpal tunnel syndrome. 00:09 Carpal tunnel syndrome is the most common focal peripheral neuropathy. 00:13 It happens when you have a compression of the median nerve as it innervates the wrist and goes through the transverse carpal ligament. 00:21 Here is a sign of the radial, ulnar, and median nerves. 00:26 Here’s another representation showing where the median nerve goes and how it’s going to affect the hand. Carpal tunnel syndrome occurs with repetitive hand motion. It is something that the median nerve will innervate lumbricals 1 and 2, the opponens pollicis, the abductor pollicis brevis, and the flexor pollicis brevis. 00:52 We use the mnemonic Meat-LOAF to remember that the median nerve innervates these muscles. 00:56 These are also the muscles that would atrophy when carpal tunnel syndrome gets bad. 01:02 It’s also where you’re going to feel the symptoms of tenderness, numbness and weakness. 01:07 If caught early, carpal tunnel syndrome can be treated, and surgery can be avoided, and damage to the muscles can be avoided. 01:16 Who gets carpal tunnel syndrome? We see it in people when they gain a lot of weight. 01:21 We see it in patients who are pregnant. 01:23 We see it with specific activities, a lot of typing or a lot of hand use. 01:27 We also see it in hypothyroidism and diabetes; when you have dehydration. 01:32 People can get a traumatic carpal tunnel syndrome from swelling. 01:35 People with malignancy can have swelling in the carpal tunnel as well. 01:38 The symptoms of carpal tunnel syndrome are typically pain, pain and numbness in the distribution area of the median nerve. 01:47 The numbness stays there. It goes tingling and it gets worse. 01:51 It’s usually worse at night and it's usually often relieved with a flicking or a reversing of the exact motions that cause the carpal tunnel syndrome. 02:03 So we often call the hand flicking self OMM. 02:07 When someone comes with symptoms of carpal tunnel syndrome, we have to worry about cervical radiculopathy or chronic tendinitis, a pronator teres syndrome or any of these other conditions that can cause symptoms similar to carpal tunnel syndrome. 02:21 Once you’ve ruled out these other symptoms mostly through physical exam, you can move forward and figure out how to treat it. 02:30 You want to confirm with a physical test, a physical diagnostic test. 02:33 It’s called Phalen’s where you put the wrist together at 90 degrees and hold it for about one minute and seeing if you reproduce the symptoms of paresthesias, of numbness and tingling in the fingers. 02:45 The other test that we commonly do is called Tinel’s sign. 02:48 You take two fingers and tap over the median nerve. 02:52 You see if you get a shooting pain of reproduction of the paresthesias and of pain in the area of the median nerve. 02:59 When you examine the patient, you may notice thenar atrophy if the patient’s had a carpal tunnel syndrome for a while. 03:08 There may be weak abduction of the thumb. 03:11 You may also notice a decrease in two point discrimination because of the swelling’s effect on the nerve. 03:17 We can also give a questionnaire to a patient to find out about their symptoms. 03:22 We can do electrodiagnostic testing to see if there’s delayed conduction or slowing of nerve conduction through the median nerve. 03:30 Those are definitive tests for carpal tunnel syndrome. 03:33 The osteopathic considerations include ruling out upper thoracic somatic dysfunction, carpal tunnel somatic dysfunction, and a viscerosomatic reflex involving the myocardium, the lungs, and the esophagus. 03:48 If you use the five models approach of evaluating a patient, you can look at both respiratory-circulatory model and the neurologic model to explain what’s going on here. There are biomechanical issues as well. 04:02 Biomechanical thinking of the impingement of the median nerve is also part of what’s going on. OMT is a very common and very effective treatment that will reduce the myofascial restrictions going on. 04:15 It includes self stretching as well as stretching by the OMT provider of the area. 04:21 There are three techniques we want to go over. 04:24 There will be videos of these that you can look at as well. 04:27 The first is a myofascial release technique. 04:30 In the myofascial release technique, you put your fourth and fifth digits of both hands between the patient’s fourth and fifth digits. 04:39 So you hold the hand. You extend it slightly and then you can treat the area. 04:45 You dorsiflex the wrist and then you stroke the area allowing for enhanced motion. 04:53 I will show you a video so you can see it better. 04:57 The next technique is the opponens rolls maneuver. 05:01 This is when you take the thenar carpal ligament and you work to release it by grasping the patient’s thenar and hypothenar areas. 05:09 Then you pull on the thenar area internally while moving the thumb into extension so you create some traction to that space. 05:19 Again there’ll be a video of the opponens rolls maneuver. 05:22 The last technique is called the bilateral thumb pressure technique. 05:26 In this technique, you hold the distal forearm with the thumbs on both sides. 05:32 You contact the anterior aspect of the forearm muscle and the interosseous membrane while the fingers grasp the posterior aspect of the forearm. 05:41 Once you have that patient locked up, you want to exert a gentle force ventrally to engage the soft tissue. 05:49 You do that in a motion towards the head and you roll out laterally until the barrier of tissue motion is reached. 05:57 We’ll have a video of this one as well. 06:00 In addition, treatments with NSAIDS are used. Wrist splinting will limit use and give this patient a good sense of when the symptoms are developing and what needs to be done. You get more worried if there is increased sensory loss or prolonged motor latencies, if numbness and tingling doesn't go away and stays there all the time, and if you see thenar or hypothenar atrophy. 06:25 Those are signs of worsening of carpal tunnel syndrome. 06:28 Again, carpal tunnel syndrome is a common condition. 06:31 It’s an overuse condition. It’s a condition that osteopathic medicine has a lot to offer. 06:36 These were the treatment methods for carpal tunnel syndrome. 06:40 I hope you find it useful. Thank you.
About the Lecture
The lecture Carpal Tunnel Syndrome by Tyler Cymet, DO, FACOFP is from the course Osteopathic Treatment and Clinical Application by Region. It contains the following chapters:
- Carpal Tunnel Syndrome
- Myofascial Release Technique
- Opponens Roll Maneuver
- Bilateral Thumb Pressure Technique
- First Line of Treatment
Included Quiz Questions
Which of the following structures does the median nerve innervate? (Select all that apply)
- 1st and 2nd Lumbricals
- Abductor pollicis brevis
- Flexor pollicis brevis
- Opponens pollicis
- Extensor pollicis brevis
Which of the following special tests are used in the assessment of carpal tunnel syndrome? (Select all that apply)
- Tinel's sign
- Phalen's test
- Reverse Phalen's test
- Finkelstein's test
- Cozen's test
Which of the following osteopathic techniques could be used to treat carpal tunnel syndrome? (Select all that apply)
- Myofascial release technique
- Opponens roll maneuver
- Bilateral thumb pressure technique
- Spencer technique
Author of lecture Carpal Tunnel Syndrome

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
