Playlist
Show Playlist
Hide Playlist
Cesarean Section (C-Section)

-
Slides CesareanSection Obstetrics.pdf
-
Download Lecture Overview
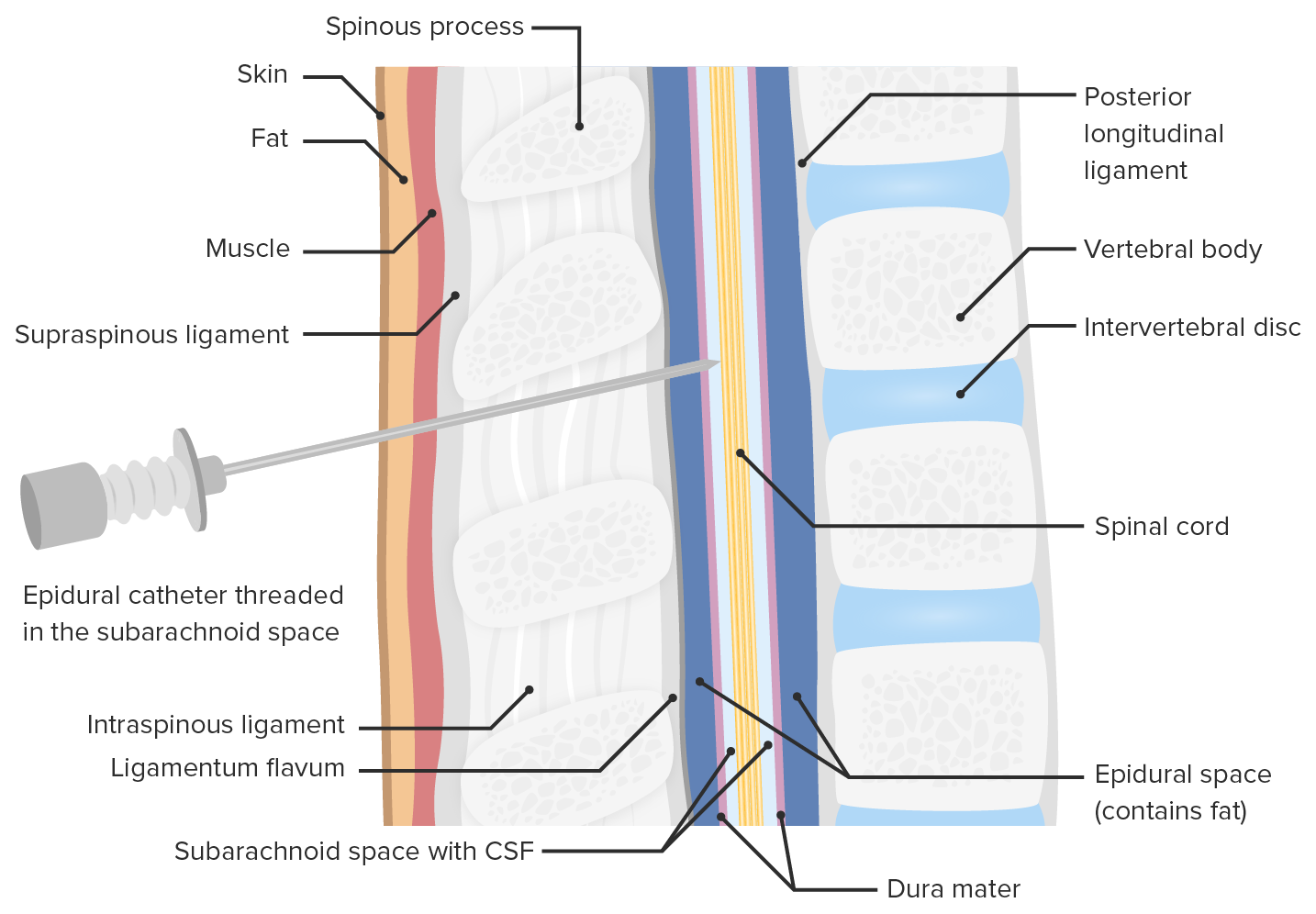
00:01 Now we'll talk about Cesarean section. 00:05 So what is the indication for C-section? It can be fetal intolerance of labor. 00:09 Meaning a Category 3 tracing. 00:12 Arrest of dilation or descent in labor. 00:15 Meaning the cervix doesn't dilate after 2 hours or the baby doesn't descent after 2 hours when they are in the second stage of labor. 00:22 Malpresentation such as breech. 00:24 Placental abnormalities such as placenta acreta, increta or percreta. 00:29 And previous uterine surgeries such as myomectomy. 00:32 Or if a patient has had more than two C-sections. 00:36 For C-section techniques, let's first talk about anesthesia. 00:41 Now this is discussed in more detail in another lecture. 00:43 But let's briefly talk about it here. 00:45 So there's three options. 00:46 Epidural, spinal or general. 00:48 With epidural, the anesthesia is placed in the epidural space through a catheter allowing for continuous pain relief. 00:56 Generally used for labor in patients. 00:59 Spinal is one injection into the subarachnoid space. 01:02 This last approximately 2 to 4 hours. 01:04 With general anesthesia we only perform this in an emergency. 01:12 Next let's talk about the type of skin incisions we can have during a C-section. 01:16 First is Pfannestiel. 01:18 That's what is demonstrated here in this picture. 01:20 With Pfannestiel there is less risk of dehiscence. 01:24 Cosmetically is preferred. 01:27 But the downside there's not as much as exposure to the abdomen as when we see a midline incision. 01:34 With midline you have a faster entry into the abdomen. 01:37 There's less blood loss. 01:39 However, the downside is a higher rate of dehiscence. 01:44 So let's talk about the layers that we go through when we are performing a C-section. 01:48 First we go through the fascia. 01:51 After the fascia is opened, we see a rectus abdominal muscles. 01:55 You can see them displayed here. 01:57 Those are separated and we identify the peritoneum. 02:01 Once the peritoneum is entered, then we make it to our uterus. 02:05 So with our uterine incisions there's a few options there. 02:10 Low transverse is the most common uterine incision. 02:13 Because the incision is made in the lower uterine segment, the non-contact top part of the uterus. 02:18 This is the least likely to rupture. 02:20 So if a patient have had one C-section, she is a candidate for trial of labor after cesarean. 02:26 And there is a low risk of rupture. 02:28 Less than 1%. 02:30 Low vertical incision is utilize if the fetus is in a presentation such as transverse back down that would not allow delivery through a low transverse incision. 02:41 Classical incisions are utilized when C-section is performed at an earlier gestation. 02:46 And the lower uterine segment has not developed or has not thinned out. 02:51 And then T-incision is an upward extension of the low transverse incision when there's difficulty delivering the baby. 02:57 Now this incision has a highest risk of rupture during subsequent pregnancies if labor occurs. 03:03 The only type of uterine incision where we do evocate for a vaginal birth after cesarean or a trial of labor after cesarean is the low transverse incision. 03:15 Now let's talk about repair of the hysterectomy. 03:19 Now this is done in one or two layers. 03:21 And the big part of the repaired of the hysterectomy, the most important part is we need to maintain hemostatsis.
About the Lecture
The lecture Cesarean Section (C-Section) by Veronica Gillispie, MD, MAS, FACOG is from the course Intrapartum Care.
Included Quiz Questions
What is the most important part of repairing a hysterotomy?
- Maintaining hemostasis
- Tucking in all the endometrium
- Avoiding the uterine serosa
- Trying to complete the repair in one layer
- Assuring the repair is done with interrupted vertical mattress pattern
History of which of the following types of uterine incisions is the safest to attempt labor and vaginal delivery (ie. a VTOL) in future pregnancies?
- Low transverse hysterotomy
- Classical hysterotomy
- Low vertical incision
- T-incision
- J-incision
What are the advantages of the Pfasnnenstiel incision when compared to a midline skin incision?
- Better cosmetic result
- More exposure for delivery of the fetus
- Faster operative time
- Less blood loss
- Higher rate of wound dehiscence
For which of the following patients a vaginal trial of labor can be an option?
- A 34-year-old woman with a history of 1 c-section (low transverse incision) for the arrest of dilation during labor
- A 35-year-old woman with a history of 3 prior c-sections at term. The first two sections were due to fetal intolerance during labor, and the third was due to the arrest of the second stage of labor
- A 28-year-old woman with a history of 1 prior c-section (classical incision) at 27 weeks for life-threatening fetal abnormality
- A 27-year-old woman with a history of fundal fibroid myomectomy
- A 31-year-old woman with a history of 1 prior c-section (low vertical incision) for transverse backdown fetal malpresentation
Author of lecture Cesarean Section (C-Section)

Veronica Gillispie, MD, MAS, FACOG
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
