Playlist
Show Playlist
Hide Playlist
Bradyarrhythmias: Three Degrees of AV-Block

-
Emergency Medicine Bradycardia.pdf
-
Download Lecture Overview
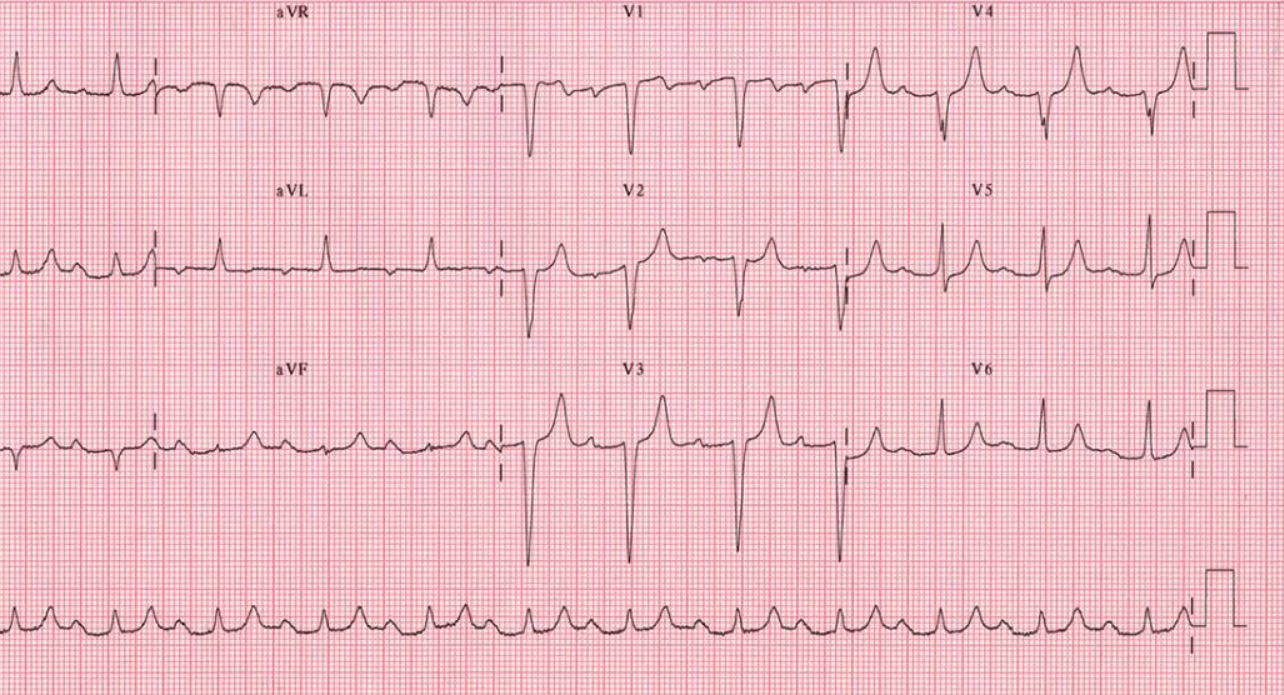
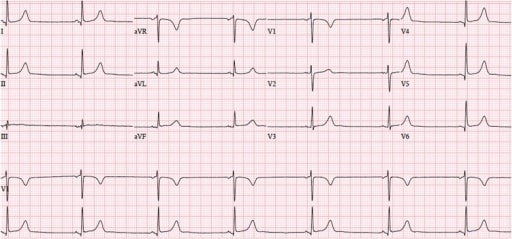
00:00 Alright, let’s move on now to first degree AV block. 00:03 So once again we have normal P waves and the Ps on this rhythm strip are marked. 00:09 We have normal QRS complexes and we have a 1:1 P to QRS ratio just like we did in Sinus bradycardia. 00:17 The big difference here is that now our PR interval is prolonged, so the PR interval is greater than 200 ms, in this particular strip it’s 240 ms so eEvery P wave has a QRS following it, there's a one to one ration between Ps and QRSs but the interval between the P wave and the QRS is prolonged. 00:40 That PR interval once again is gonna be constant however for beat to beat. 00:44 So, first degree AV block is typically located in the AV node. 00:51 It’s a problem of nodal refractoriness where the node -- where conduction through the node is slow or inefficient. 01:00 This is actually nonpathologic in many cases and 2% of completely normal healthy adults have first degree AV block their entire lives and it doesn’t cause any clinical manifestation. 01:12 It can also be caused by AV nodal blocking agents. 01:16 Again, no treatment is typically needed for this in the emergency setting although you would want to avoid the use of drugs that might exacerbate it. 01:25 Now, let’s move on to second degree AV block, Mobitz Type I, this block is also known as Wenckebach. I'm not really sure why it has two names but we’ll call it Mobitz I here. 01:36 Now, in Mobitz I, you once again have normal P waves; so you can see the Ps are marked on this rhythm strip, they're normal in appearance and they come along at regular intervals. You also have normal QRS complexes which are also noted on the rhythm strip. 01:51 However, we have progressive prolongation of the PR interval from beat to beat so you can see the first beat on the rhythm strip, the PR interval’s a 140 ms which is normal. 02:05 The second beat on the rhythm strip, the PR interval is up to 240 ms so it’s gone from normal to prolonged and then check out the third beat, now we have the P wave but there’s no QRS complex following it, we've dropped a QRS complex and then at the next beat the cycle resets itself and we're back once again to a short PR interval. 02:29 So, Mobitz type I or Wenckebach is again a disease of nodal refractoriness, so the problem here is that you have difficulty conducting through the AV node. 02:42 In that first beat the conduction is normal, however for the second beat, the AV node is a little bit more refractory and it takes more time for the impulse to transmit through the AV node and produce a QRS complex. 02:55 On that third beat, the node is now completely refractory, the impulse can't get through to the ventricle and the QRS complex is dropped, so again, this is a problem within the AV node related to refractoriness. 03:11 The causes of this include again, increase parasympathetic tone so some patients can have this just in the setting of having very high vagal tone, it could be precipitated by AV nodal blocking agents but you can see it in the setting of cardiac ischemia or other cardiac disease. 03:30 You typically will see this in association with inferior myocardial infarctions and usually it’s a transient finding with a pretty good prognosis, so Mobitz type I blocks do not typically progress to higher grade heart block. 03:43 They typically resolves spontaneously when they are caused by underlying pathology and you usually don’t need to do much in the way of treatment. 03:52 Now, if you're concerned that your patient is having cardiac ischemia or another acute cardiac illness, you probably wanna make sure that you have transcutaneous pacing available, we're gonna talk a little bit more about that as we go through but otherwise you don’t really need to do much for these patients in the emergency setting, except be prepared in the event that they do deteriorate. 04:14 Alright, now we're gonna move on to the more sinister heart blocks. 04:17 So this is our Mobitz type II AV block. 04:21 So again, our P waves are normal so you can see the P waves, they have normal in morphology, they're coming along at regular intervals throughout the rhythm strip. 04:34 We also have normal QRS complexes which are marked here. 04:37 We have consistent PR intervals from beat to beat so you can see, for each beat, the PR interval is the same, 160 ms, a 160 ms, 160 ms -- but look what happens here, on this next after this next P wave -- now we have a dropped QRS complex. 04:57 So we have constant PR intervals, the same PR interval from beat to beat and then we have one all of a sudden that’s not transmitted, we have a dropped QRS. 05:08 So, Mobitz II is a problem below the level of the AV node and if you think about it, it makes sense. 05:16 You have a constant and normal PR interval so AV nodal connection is normal; this is not a problem in the node because you're able, for every transmitted beat to conduct normally and consistently through the node. 05:28 This is a problem at or below the level of the Bundle of His. 05:31 It can be caused by simple degeneration, with aging; it can be caused by cardiomyopathy but when we see it in the acute setting, its most commonly associated with ischemia in particular Anteroseptal Myocardial infarctions. 05:47 And in this case because you're dealing with pathology that’s actually injuring the portion of myocardium where the conduction system lives, it actually is unlikely to reverse itself, it has a poor prognosis without treatment, so patients with Mobitz II type blocks often will not get better spontaneously and end up needing a permanent pacemakers placed. 06:11 You can also see Mobitz II with some drugs and toxins particularly nodal blocking agents in pathologic doses or overdoses. 06:22 The treatment for Mobitz II is once again be ready to pace this patient. 06:27 Now unlike Mobitz type I, were the need for pacing is sort of a theoretical risk, you're almost never gonna need to do it -- these patients can deteriorate into complete heart block, they can become hemodynamically unstable and you really wanna make sure that you are ready to manage them in the event that they do become unstable. 06:46 So you're gonna implement transcutaneous pacing if they're unstable right now, if they're not you're gonna prepare to do it and you also wanna prepare to place a transvenous pacer should that become necessary and we’re gonna talk more about how pacing is conducted at the end. 07:02 Alright, we're gonna move on to our final and most serious heart block now, this is our third degree or complete AV block. 07:10 In third degree heart block you can see we have normal P waves and these Ps come along at regular intervals, the PP intervals from atrial beat to atrial beat is normal. We also have normal QRS complexes, now. 07:26 In some cases the QRS can be wide but the QRS rate should be regular so the QRSs should come along at regular intervals from one beat to the next. 07:36 You can see we have normal PP intervals so the atria are beating at a normal and regular rate. 07:43 We also have normal RR intervals so the QRS complexes are coming along at a regular rate. 07:50 However, there's no meaningful relationship between the P waves and the QRS complexes, so if you look the P waves are kinda doing their thing, the QRS complexes are kinda doing their thing but there's not a reliable relationships between the two and this is because there’s complete dissociation between the activity of the atria and the activity of the ventricles. 08:15 Now, this is really problematic, this again is gonna almost always be located below the level of the AV node, at or below the level of the Bundle of His and its associated with the same kinds of pathology that caused Mobitz type II blocks. 08:31 These patients can often be very sick because they have no transmission through the AV node they're relying on some ectopic pacemaker to keep their ventricles beating so because nothing is going through the AV node, they're relying on a back up pacemaker in the heart, the junctional pacer or ventricular pacer to keep their heart beating. 08:55 So these patients can often have very, very, slow heart rates that are inadequate to support their perfusion. 09:01 So once again, we wanna be ready to pace these patients immediately, we wanna initiate transcutaneous pacing right away if the patient is unstable, otherwise, we wanna be prepared for it and we wanna be prepared for placement of a transvenous pacer. 09:16 So, when is bradycardia an emergency? When are we gonna really wanna gonna aggressively treat bradycardic patients in the ED? We’ll much like we talked about for tachycardia it all comes down to their clinical stability. 09:30 So if the patient is hypotensive, if they're not maintaining normally or if they have evidence of cardiac ischemia, these are patients who we want treat more aggressively up front and get their heart rate back up to a physiologic level.
About the Lecture
The lecture Bradyarrhythmias: Three Degrees of AV-Block by Julianna Jung, MD, FACEP is from the course Cardiovascular Emergencies and Shock.
Included Quiz Questions
Which of the following does NOT describe a first-degree AV-block?
- PR interval < 200 ms
- Normal P wave
- Normal QRS complex
- 1:1 P:QRS ratio
- PR interval is constant
Which of the following does NOT describe a Mobitz I block?
- A third-degree AV-block
- Normal P wave
- Normal QRS
- Progressively longer PR intervals
- Dropped QRS complex
Which of the following does NOT describe a Mobitz II block?
- Progressive PR interval prolongation
- A second-degree AV-block
- Normal P wave
- Normal QRS complex
- Dropped QRS complex
Which of the following does NOT describe a third-degree AV-block?
- P wave always precedes a QRS complex
- Normal P wave
- Normal to wide QRS complex
- Normal P-P interval
- Normal R-R interval
Which of the following statements regarding heart blocks is INCORRECT?
- Emergency treatment is always necessary for first-degree AV-block.
- Mobitz II AV blocks are usually located below the AV node.
- Third-degree AV-blocks can be caused by anterior myocardial infarction.
- AV-nodal blockers are contraindicated in second-degree AV-block.
- Mobitz I AV-blocks are located within the AV node.
Author of lecture Bradyarrhythmias: Three Degrees of AV-Block

Julianna Jung, MD, FACEP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
