Playlist
Show Playlist
Hide Playlist
Atypical Ductal Hyperplasia

-
Slides BenignBreastDiseases Surgery.pdf
-
Download Lecture Overview
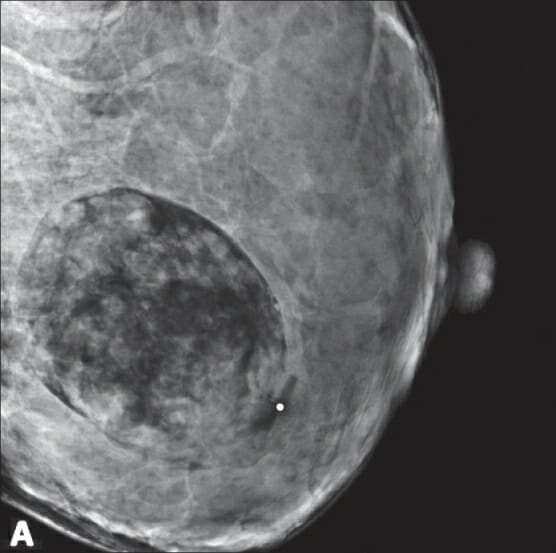
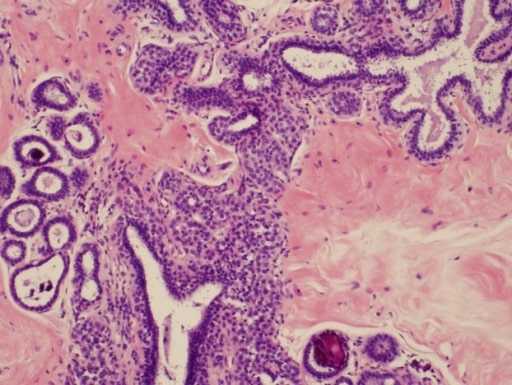
00:01 Let’s move on to a discussion of atypical ductal hyperplasia. Remember, ADH or atypical ductal hyperplasia is considered a proliferative disease and may infer increased risk of cancer, proliferation of cells and histologically very similar to in-situ cancer. However, atypical ductal hyperplasia in and of itself is not considered premalignant. There is however, an increased risk of breast cancer three to five fold in the general average population. And it’s usually discovered incidentally on biopsy of either a palpable mass or a mammographic abnormality. 00:38 Remember, these are incidental findings. Here’s a mammogram of an atypical ductal hyperplasia. 00:48 It is difficult to distinguish based on the mammogram alone. Again, as a reminder, typically when mammogram showed microcalcifications or suspicious lesions, patients undergo some type of biopsy. When the biopsy result shows atypical ductal hyperplasia, it does not necessarily explain the microcalcifications. For biopsies, if it’s a palpable lesion, one can again do a core needle biopsy. If it’s not palpable, one can send the patient for a stereotactic biopsy where 3D reconstructions guide an automated machine to biopsy the lesion. This stereotactic biopsy minimizes the need for an excisional biopsy or incisional biopsy in the operating room. 01:35 The question is, is surgery needed for atypical ductal hyperplasia? The answer is no. If a biopsy result shows atypical ductal hyperplasia, no excision is needed as the lesion itself is not premalignant or malignant. However, remember it confers increased risk of invasive cancer and that should be told to the patient in counseling. The patient may also be responsive to hormonal therapy. 02:02 Here in risk reduction, estrogen receptor modulators such as tamoxifen may be given to patients with atypical ductal hyperplasia to decrease the risk of invasive cancer. Here are some important clinical pearls and high-yield information. Do not assume that all mammographic abnormalities are malignant. Similarly, if a mammographic abnormality is demonstrated and the biopsy result shows a benign lesion, perhaps more biopsies are needed. Excision is not necessary in atypical ductal hyperplasia. But because this is a proliferative form of benign breast disease, it infers increased risk to the patient. Estrogen receptor modulators may be used to decrease risk of invasive cancer. Thank you very much for joining me on this discussion of benign breast disease.
About the Lecture
The lecture Atypical Ductal Hyperplasia by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Which of the following statements about atypical ductal hyperplasia is FALSE?
- Atypical ductal hyperplasia is considered a premalignant lesion.
- Atypical ductal hyperplasia is a proliferative breast lesion.
- Atypical ductal hyperplasia confers up to five times increased risk of breast cancer.
- Atypical ductal hyperplasia is often an incidental finding on pathology.
- Atypical ductal hyperplasia usually doesn't require surgical excision for treatment.
Which of the following is recommended to decrease the risk of invasive breast cancer in a patient with diagnosed atypical ductal hyperplasia?
- Estrogen receptor modulators (i.e. Tamoxifen)
- Simple excision of the lesion
- Wide local excision of the lesion
- Bilateral prophylactic mastectomies
- Repeat mammograms every 6 months to monitor the growth of the lesion
Author of lecture Atypical Ductal Hyperplasia

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
