Playlist
Show Playlist
Hide Playlist
Asthma: Signs and Symptoms




-
Slides ObstructiveLungDisease Asthma RespiratoryPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
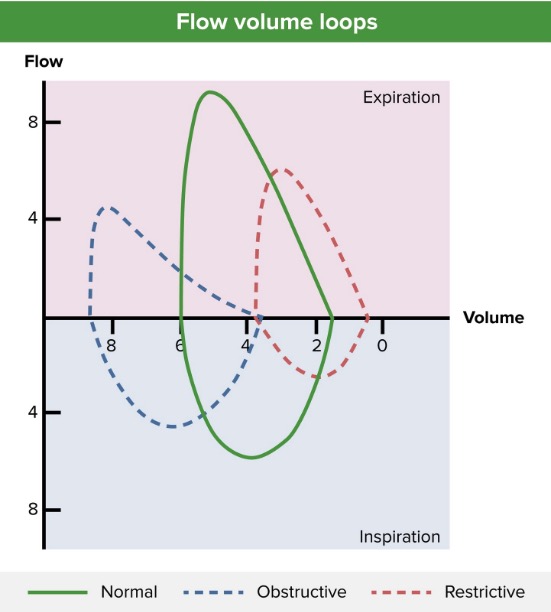
00:00 Asthma is an obstructive, expiratory disease as noted, patients will have episodic wheezing, cough and dyspnoea. Now, you can have cough variants of these and these “cough variants” or cough and primary symptom characterize by coughing “fits” or can be induced by viral infection. So these coughing fits, some patients have a cough variant of asthma as I said earlier well perhaps exacerbated by a previous upper respiratory tract infection perhaps viral or this coughing “fits”. 00:32 Nocturnal cough is dangerous. So, if a patient suffering from asthma has nocturnal cough then you should consider this patient who’s never been treated. Untreated is your issue. 00:45 Now that could be very, very dangerous. If asthma goes on to be untreated you can only imagine that there’s increase mucous production. And so therefore now, the patient has difficulty with ventilation. Wow. So now this puts you in the realm of, type 2 respiratory failure which means what exactly? Well, the patient’s already hypoxic we knew that. Hypoxemia set in at PO2 of being less than 60, but then there might be hypercapnic upper respiratory failure. 01:18 And at some point if the patient is untreated for this asthma, the patient is always vulnerable to severe asthma attacks and we call that status asthmaticus. 01:30 Let’s take a look at the flow volume loops or the loop spirometries. Things that we have become quite accustomed to. Once again, on your left, this is perfectly normal. What then represents the bottom half represents the inspiration and your x-axis here represents your volume. What is it called when you have full inspiration and you filled up your lungs? This is then referred to as being your total lung capacity. The top half of the curve which is what you’re paying attention to specifically and I’ll show you next, well, that would be exhalation. 02:10 In asthma, which is obstructive, you’ll then notice please, that there’s going to be an increase in total lung capacity when compared to normal and most importantly upon expiration you’ll notice that first and foremost you won’t be able to reach peak expiration and the fact that you have a scalloped type of formation or pattern upon further exhalation. Remember the entire top half represents exhalation. You probably want to divide that into the first half, and the second half, and what you always have left over is your residual volume. But in a patient with asthma, with obstructive, then it would be a scalloped portion. Now, before we move on, you tell me what the FEV1/FVC ratio is? Good, decreased, always. This is obstructive. I’ll tell you when it’s normal.
About the Lecture
The lecture Asthma: Signs and Symptoms by Carlo Raj, MD is from the course Obstructive Lung Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is not seen in the pathogenesis of asthma?
- Decreased smooth muscle tone
- Increased smooth muscle tone
- Increased inflammation
- Increased mucus production
- Increased edema
Which of the following is the correct representation of the flow volume loop in asthma?
- Obstructive loop, shift to the left
- Obstructive loop, shift to the right
- Restrictive loop, shift to the left
- Restrictive loop, shift to the right
- Obstructive loop, bilateral shift
Author of lecture Asthma: Signs and Symptoms

Carlo Raj, MD
Customer reviews
3,0 of 5 stars
| 5 Stars |
|
0 |
| 4 Stars |
|
0 |
| 3 Stars |
|
1 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Its an ok explanation. Should be more detailed and not presume that the studends know certain things! Also, more exercises should be proposed
