Playlist
Show Playlist
Hide Playlist
Wilson's Disease

-
Slides GD liver disease.pdf
-
Download Lecture Overview
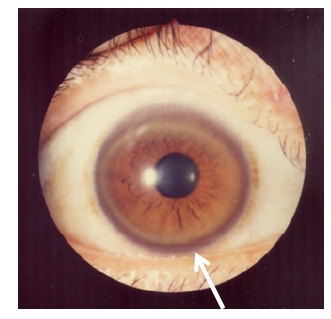
00:01 We'll go into our second metabolic disease of the liver and this is Wilson's disease. 00:07 As soon as you hear Wilson, close your eyes, you're telling me what element? Copper, copper, copper. That's where you begin. 00:15 Hemochromatosis, which element? Iron, iron, iron. Pathology? Wilson, the copper is causing damage, once again, from head and down to your liver. 00:26 If copper accumulates in basal ganglia, what do you look like? And what's your walk? Shuffling gate. What about your flexion of the elbow? Cogwheel rigidity. What is all this? It's a sign often a lot like your Parkinson, but it's not Parkinson. 00:53 It's Parkinson-like, right? Be careful. 00:56 So, the copper here is accumulating basal ganglia giving you the symptoms in your patient of Parkinsonism. 01:01 What's the topic here? Liver disease. 01:04 So, copper accumulating in liver causing death of the liver. 01:08 Let's talk about pathogenesis. It's important. It's an autosomal recessive. 01:13 Excess of accumulation of what kind of copper? What do you mean what kind of copper, Dr. Raj? I mean copper's copper. No, in the body, you have either bound or free. 01:24 Which faction of copper is elevated? What's this copper accumulating in the basal ganglia? In the liver and so forth? Free copper. Why? Why? Why? The liver is missing the binding protein for copper. 01:40 You remember what the name of that is? We'll see. 01:44 All right, presents in under age of 40? You're right. I know you are. 01:48 Well, let's just make sure we're -- you know, we have the full picture first. 01:50 Age, about 40, young, hemolytic anemia, jaundice, elevated ALT, fulminant liver failure, neurological symptoms. 01:58 There you have it. Free copper accumulating in different places. 02:02 Neurologic, I talked about Parkinson-like liver disease. 02:06 Unfortunately, death to the liver. 02:09 The patient might have issues with hemolytic anemia and jaundice as well. 02:14 I'll show you a picture of Kayser-Fleischer, in which you have free copper accumulating in the descement membrane of the cornea. 02:21 It is nearly 100% sensitive in presence of neurologic symptoms. 02:25 Okay. So, just before we move on, I know it's killing you, in terms of what is being deficient from the liver in Wilson's disease. 02:35 What is copper bind to? Ceruloplasmin. 02:38 That's your pathology in Wilson's disease. 02:42 Let's take a look. Kayser-Fleischer, the areas that you're seeing that are brown are the areas that is accumulation of copper. 02:52 Kayser-Fleischer. This patient had Parkinson-like symptoms. 02:58 No doubt, this patient had Wilson's. 03:02 What kind of free copper did you find in the serum? Increased, increased, increased. 03:07 I'm gonna talk -- I'm gonna walk you through, step by step by step, of the labs that's important for you with Wilson's. 03:13 But your diagnosis will come mostly just by paying attention to your patient. 03:18 Let's now walk you through the laboratory test, pathogenesis, and diagnosis of Wilson's disease. 03:24 The liver fails to synthesize ceruloplasmin. 03:29 Would you be able to tell me the concept of total? Total means free plus bound. 03:36 What is ceruloplasmin to you? Bound. 03:39 What faction or what component of your total makes mostly your total? Free or the bound? The bound, the bound, the bound determines the total. 03:50 Okay. Now, with all that in mind that we walked through plenty of times, if you have low ceruloplasmin and you know that's the bound form, then what's your bound levels in Wilson's? Bound copper is decreased. Clear? If you're bound is decreased and you know that that is the major constituent of total, then what's your total? Decreased. 04:13 Keep going. So, if your bound is decreased, your total is decreased, then what has to be elevated? The free. 04:20 So, Dr. Raj, why isn't free -- why isn't total increased if the free is total? I just told you that if you're thinking total, the bound is the major constituent. 04:30 So, you will have increase in free, no doubt. 04:33 That free copper then accumulates from -- like we talked about. 04:36 Kayser-Fliescher, we talked about basal ganglia, so therefore, Parkinson-like and then here, obviously there's going to be liver damage, and then where would you find this free copper? In the urine. Okay? Excretion in the urine. Free copper. Liver biopsy with high free copper content. 04:54 What about your ceruloplasmin? Low. What about the bound? Low. 04:59 What about the total? Low. 05:01 Management. What do you wanna do? Penicillamine is the drug that you should be thinking. It's a chelator. 05:10 You need to remove the copper. 05:12 Remember in hemochromatosis, what were you doing? Week by week by week, phlebotamy, phlebotamy, phlebotamy, so that you can then move the iron. Zinc is used for maintenance. 05:23 Worst case scenario, once the liver has been dead, unfortunately, liver transplantation. 05:29 One would think that the number of times we've seen liver transplantation that it's easy to find a liver. 05:35 You know that's not true. It's dangerous. 05:38 All siblings should be screened because this is a genetic issue.
About the Lecture
The lecture Wilson's Disease by Carlo Raj, MD is from the course Liver Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following proteins is deficient in Wilson's disease?
- Ceruloplasmin
- Sphingomyelinase
- Galactosidase
- Glucocerebrosidase
- Arylsulfatase
Which sign or symptom has the highest sensitivity for the diagnosis of Wilson's disease with neurological symptoms?
- Kayser-Fleischer rings
- Golden color of skin
- Increased ALT
- Pruritus
- Icterus
What is the structure in the brain where copper accumulation resulting from Wilson’s disease MOST commonly occurs?
- Basal ganglia
- Uncus
- Hippocampus
- Medulla
- Cerebellum
What is the structure in the eye where copper accumulation resulting from Wilson’s disease occurs?
- Descemet's membrane
- Iris
- Anterior chamber
- Pupils
- Lens
Which of the following laboratory findings is seen in Wilson's disease?
- Increased urinary copper
- Decreased urinary copper
- Increased ceruloplasmin
- Increased stool copper
- Decreased stool copper
Which of the following laboratory findings would be expected in a patient with Wilson's disease?
- High urinary copper levels
- Liver biopsy - decreased free copper
- High bound copper levels
- Low free copper levels
- High ceruloplasmin levels
Which of the following does NOT play a role in the treatment of Wilson's disease?
- Phlebotomy
- D-penicillamine
- Trientene
- Zinc maintenance
- Liver transplant
Author of lecture Wilson's Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
