Playlist
Show Playlist
Hide Playlist
Vascular Anatomy – Blood Vessels and Pressure (Hemodynamics)

-
Slides BloodVesselsAndPressure VascularPhysiology.pdf
-
Download Lecture Overview
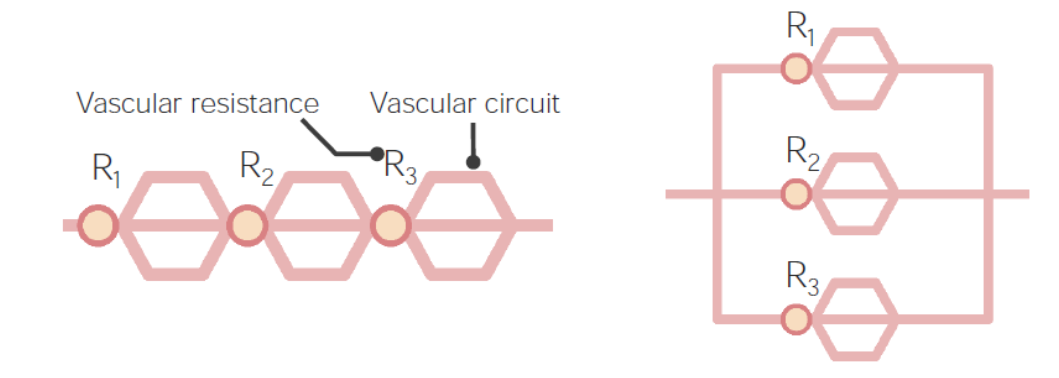
00:00 So let's take mean arterial pressure as our endpoint and go through what are the factors that affect mean arterial pressure. Well, one of the biggest things we've already discussed here is systemic vascular resistance. So the more resistance there is in the tube system, the higher the pressure. If heart rate is higher, you're going to have a higher cardiac output and that will drive pressure to increase. If the heart contracts to a greater extent, if the contractility increases which we call inotropy that will also increase mean arterial pressure. If venous compliance decreases, that will also increase mean arterial pressure. Also, if you increase the volume that's circulating around of the blood, that will increase mean arterial pressure and you usually do that through the renal sodium and water reabsorption or handling. When you go through that process, you get an increase in blood volume. By decreasing venous compliance, you get an increase in preload which is both volume and venous compliance related. 01:17 If you have an increase in preload, that also increases your stroke volume just like inotropy did. That increase in stroke volume feeds in to an increase in cardiac output just like the increase in heart rate and our final end product here is mean arterial pressure which is affected by the cardiac output and of course systemic vascular resistance. So that is why we can utilize the formula of mean arterial pressure equals or approximates cardiac output times systemic vascular resistance. So when you think about mean arterial pressure, we have to think what are the other determinants of mean arterial pressure. One of the main items to consider is how the circuit is set up and you go circuit circuit. What are we talking about with the circuit? Similar to an electrical circuit, we need to know if the blood vessels are located in series or in parallel. If you have a series circuit, series circuits have higher resistance because you have to add up each of the resistance values as you travel through a series circuit. In contrast, a parallel circuit is one in which when you open the circuit up pressure decreases because you're now putting that pressure across multiple vessels at the same time. 02:54 So between going through serial and parallel circuits, you can better understand this particular process. So here we have the normal components of a tube which is 8 times the viscosity times the length divided by pi R raised to the fourth power and now our second component is if it's arranged in a series or parallel vascular arrangement. Now, when we think about parallel arrangements, probably the easiest vessels to think about are capillaries. So if you look at a capillary structure you see that you have a single vessel starting to come in to a capillary network. Once that capillary network is open, those vessels are all in parallel to each other. 03:54 So pressure is going to dramatically decrease in a capillary because now you have this large parallel structure of vessels. That's handy when you want to drop pressure to allow for optimal exchange of various solutions. When you drop pressure like this, you also drop flow because you don't have as much of a delta P, a driving force of pressure to facilitate high flows through these vessels. Therefore, the vessels themselves have adapted to this low pressure environment. They're a lot as thick as they would be if they are in a high pressure environment and that thin vessel structure allows for better capillary exchange between the blood and the cells, whether it's to pick up metabolites and other items associated with metabolism or if it's to deliver things to be metabolized, like glucose and oxygen. So let's look at now each anatomical variant associated with the vascular tree. So we start off with a very large diameter vessel such as an aorta. We go to larger arteries and these are mainly to distribute fluid. Small arteries start to become very important for blood pressure because this is now altering the resistance of a vessel. So until this point, the aorta, the large arteries, those are conduits, they don't actually change the amount of resistance in the system to a great degree. They will not vasoconstrict, they stay at the same diameter. 05:54 Arterioles are the place in which you get the greatest drop in pressure because you can utilize resistance by changing the luminal diameter of the vessel. So this is the most important spot for having a change in blood pressure. The capillaries are there primarily just to exchange again things to be metabolized and metabolites to take away as waste products. The venules and veins, these are again to move fluid back to the heart and finally the vena cava is the largest, there is a superior and an inferior vena cava, those will drain into the right atrium. 06:40 So this completes our vascular anatomy circuit. The important ones to remember here are the arterioles, that's where the largest resistance change happens; capillaries where most of the exchange occurs and then there are other places like veins that hold a lot of the blood volume. 07:01 This graph shows you how pressures are distributed across all of these large vessels. So you can see in the aorta the pressure is really pretty high. In the arteries the pressure is still high. 07:14 The largest drop in pressure though occurs in the arterioles. In the capillaries, pressure is really pretty low. In the venules the pressure is still low. Veins and vena cava you've almost gone all the way back to zero. So you start off with a high mean pressure and then with a very very low pressure. The vena cava pressure is central venous pressure. The pressure in the aorta, that's your highest pressure. So that's why sometimes people will take mean arterial pressure minus central venous pressure because that's the largest pressure differential. Now, how does blood volume fit in to this overall scheme of controlling blood pressure? Blood volume is the amount of volume located within the vessels. Most of the blood volume is located in the venous side of the circulation. 60-80% of blood volume is located in the venous vessels. They are termed to have high capacitance, they have a high ability to take fluid and this has a handy feature because you can then cause contraction of the veins and that then can move more fluid back to the heart to increase preload and eventually increase stroke volume. You might ask what controls the venous smooth muscle? That is mainly sympathetic nervous system activation. That increases the venous tone and therefore reduces this venous volume to move it back up to the heart. The other very big principle that we would like to bring out with the blood volume distribution in the veins is that it's highly influenced by gravity. One of the best pictures we can come up with is this water balloon that's hanging. You can notice by looking at this water balloon that most of the volume is located lower rather than higher in that balloon. That is the important feature. Gravity is pulling that fluid down and unless you would resist that by squeezing it together to push that fluid back up, you would have then venous volume hanging out in lower areas. You can think of this a little bit. If you stand up and look at your feet, venous volume want to be pulling fluid down toward your feet and that case oftentimes pressure is higher in that locale and sometimes even you can get a little bit of edema formed in those areas as well.
About the Lecture
The lecture Vascular Anatomy – Blood Vessels and Pressure (Hemodynamics) by Thad Wilson, PhD is from the course Vascular Physiology.
Included Quiz Questions
Which of the following vessel arrangements will have the highest resistance across the circuit if all points of resistance are equal?
- 5 point serial arrangement.
- 3 point serial arrangement.
- 5 point parallel arrangement.
- 3 point parallel arrangement.
- 2 point parallel arrangement
Which of the following blood vessels has the largest drop in absolute blood pressure?
- Arterioles
- Venules
- Capillaries
- Veins
- Arteries
Which vessels are responsible for the exchange of metabolites?
- Capillaries
- Aorta
- Vena cava
- Femoral artery
- Brachial artery
Where does the blood in the inferior vena cava drain?
- Right atrium
- Left atrium
- Right ventricle
- Left ventricle
- Great cardiac vein
Which of the following vessels have highest capacitance and blood volume?
- Veins
- Arteries
- Arterioles
- Capillaries
- Aorta
Author of lecture Vascular Anatomy – Blood Vessels and Pressure (Hemodynamics)

Thad Wilson, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Amazing teacher, straight to the point, clear way of explaining.
