Playlist
Show Playlist
Hide Playlist
Ulnar Nerve Injury

-
Slides 05 Mononeuropathy Neuropathology II.pdf
-
Download Lecture Overview
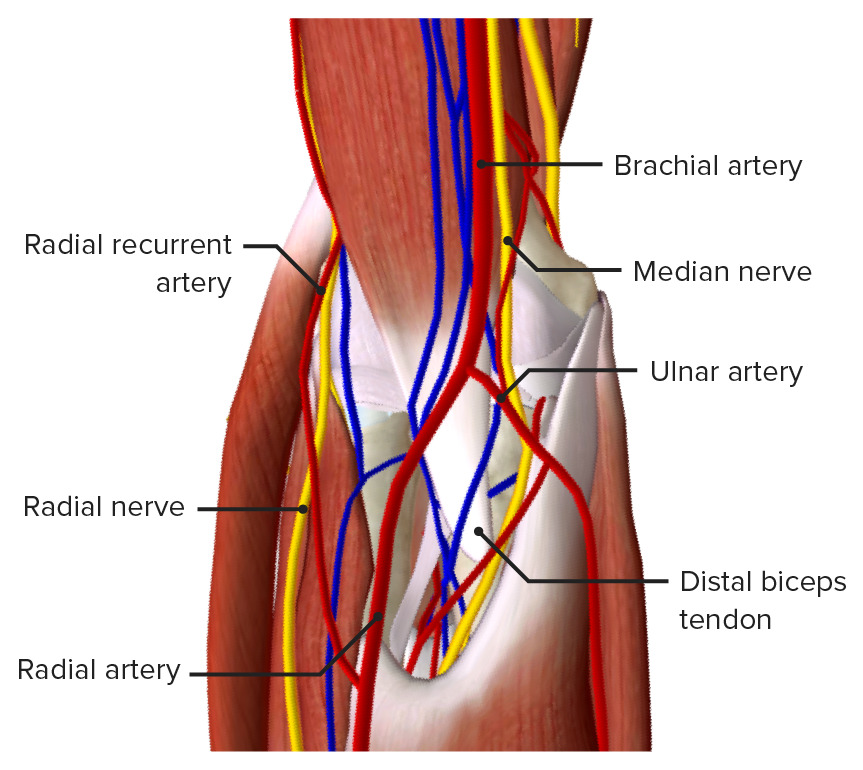
00:01 We move on to the ulnar nerve. 00:03 Take a moment here and identify the ulnar nerve. 00:05 Once again, a common site of injury. 00:07 Most frequently at the elbow, from leaning on it or trauma. 00:14 Clinical features: Weak hand. 00:16 By that, we mean once again dropping objects. 00:19 Difficulty turning keys, ignition and doorknobs. 00:22 Turning, okay? Turning. 00:26 Numbness and tingling of fourth and fifth fingers. 00:31 Anatomical position, which was my fourth and fifth. 00:34 It is the ring finger and the pinky, right? Fourth and fifth. 00:39 Where are you? Ulnar. 00:42 Medial aspect of the arm. 00:45 Wasting of the interosseous muscle. 00:49 What I wish to bring to your attention with the radial nerve, is the fact that you could have this pseudo type of interosseous issue as well and just be careful not to get the two confused, Here, it’s strictly wasting of the interossei. 01:04 The onset is usually slow, insidious. 01:08 Risk factors: More in men, diabetes, alcoholism, HIV, leaning on the elbow. 01:14 So up until the point the risk factors are pretty much across the board quite common. 01:19 Except now, specifically, leaning on the elbow. 01:23 Occupational. 01:24 For example, telephone operators or receptionists. 01:26 They don’t even realize that this is happening. 01:29 So if you’re working with too much of the hand, you’re thinking median nerve. 01:32 If you’re once again are working behind the desk, there’s every possibility that you might be spending quite a bit of time while you’re talking on the phone, leaning on the elbow. 01:42 Trauma. 01:43 For example if there’s a hitting of the elbow. 01:46 Physical examination: Look for the first dorsal wasting of the interosseous atrophy. 01:52 Test the interosseous strength. 01:53 Ask the patient to spread the fingers against resistance. 01:59 Decreased sensation to touch and pinprick over what? Fourth and fifth fingers. 02:06 Positive Tinel sign. 02:07 What does that mean to you? Tingling upon tapping the nerve at the elbow. 02:15 Spend a little bit of time with these physical exams, please, on these various mononeuropathies. 02:20 Management: Stop or once again look for lifestyle modification. 02:24 Surgery is indicated for severe lesions and for interossei atrophy due to denervation. Most common surgical option is in-situ decompression. Ulnar nerve transposition is rarely used nowadays. The success rate of in-situ decompression is acceptable. 02:42 Differential diagnosis: Here, once again, C8-T1 possibly root lesion, but usually accompanied by neck and arm pain. 02:50 ALS, amyotrophic lateral sclerosis. 02:53 Here, once again, if symptom are in more areas than just the ulnar nerve or if accompanied by speech and swallowing problems and fasciculation, all of this of course referring to ALS. 03:03 Thoracic outlet syndrome, rare but nonetheless, a differential.
About the Lecture
The lecture Ulnar Nerve Injury by Carlo Raj, MD is from the course Mononeuropathy.
Included Quiz Questions
Which of the following is most characteristic of ulnar nerve injury?
- Weak hand grip
- Wrist drop
- Positive Tinel sign
- Numbness and tingling in lateral 3.5 digits
- Defective elbow extension
Which of the following findings is NOT associated with a defect of the ulnar nerve?
- Positive Phalen maneuver
- Tingling sensation of last 2 digits
- First dorsal interossei atrophy
- Weak hand grip
- Sensory deficits in fourth and fifth fingers
Author of lecture Ulnar Nerve Injury

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
