Playlist
Show Playlist
Hide Playlist
Types of Non-Invasive Breast Cancer

-
Slides Breast Female Repro.pdf
-
Download Lecture Overview
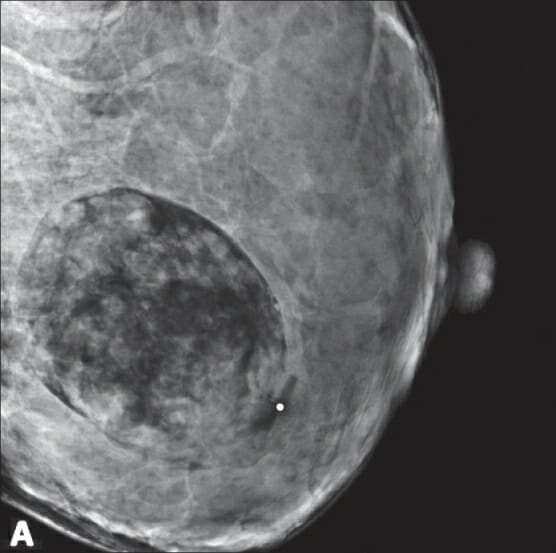
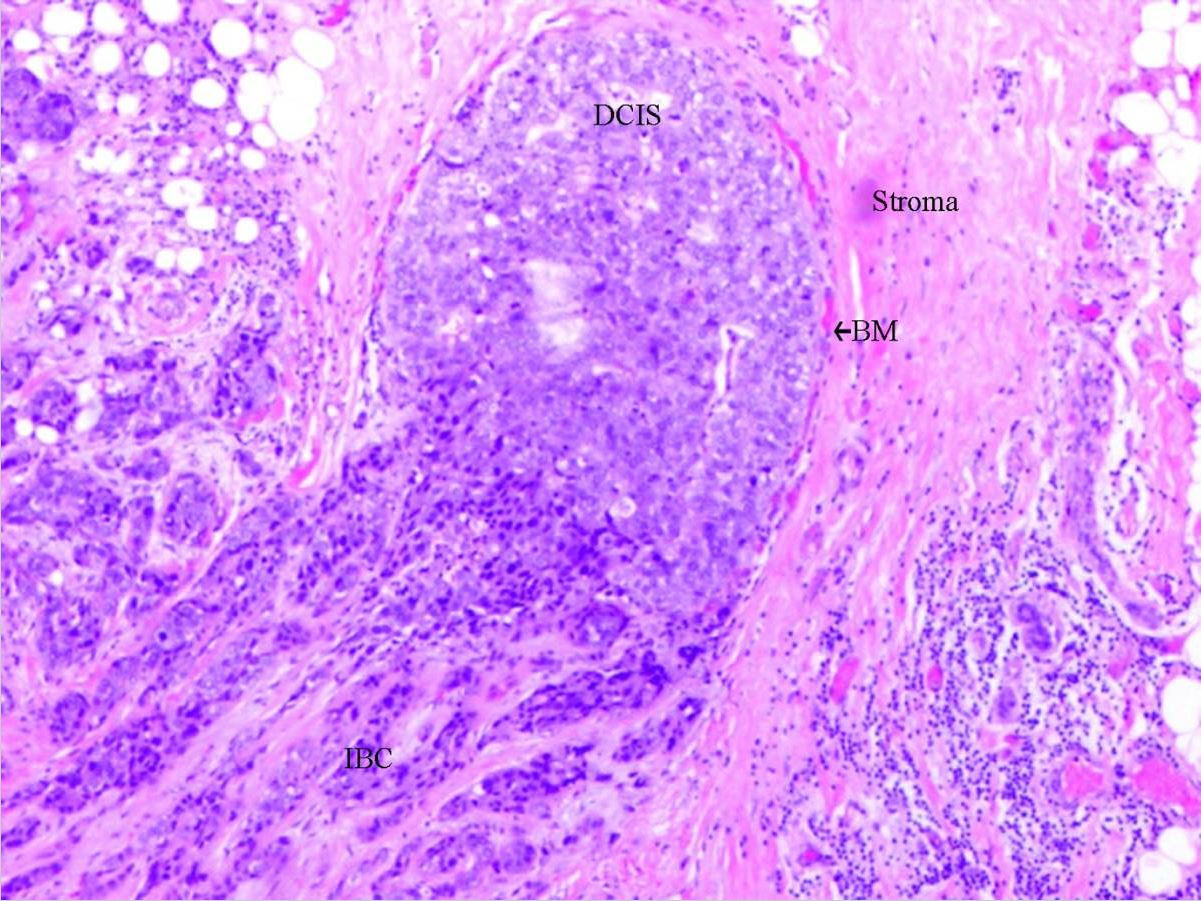
00:01 Breast cancer, the way that we will organize this for you and at this point, I’m going to give you an organization that is very much relevant to your boards. 00:10 Understand that real life clinical practice just keeps changing. 00:15 At this point, you’re not going into pathology and you’re not going into OB-GYN specifically, right? But let’s make sure that you know the basics. 00:26 We’ll begin with non-invasive breast cancer. 00:29 This is malignancy. 00:32 Our topic is in situs. 00:35 "Dr. Raj, I thought in situ meant that it was dysplasia?" No. 00:39 In situ means membrane intact. 00:41 That’s why we call it non-invasive. 00:44 Start again, breast cancer, non-invasive. 00:47 These are in situs. 00:50 After we discuss common in situs that you need to know, we’re then going to move into invasive. 00:57 What does that mean? What’s been invaded? Good. 01:01 The basement membrane. 01:05 Non-invasive number one, ductal carcinoma in situ. 01:09 So when you say ductal, what does that mean to you? You’re going from the nipple and you go into the lactiferous sinus and then you move through the major duct, the terminal duct and then lobule. 01:20 You put all the ducts together and then the duct here, unfortunately, your female has developed breast cancer. 01:26 Malignancy. 01:27 It fills the duct lumen, arises from ductal hyperplasia. 01:33 Note here early malignancy without basement membrane rupture. 01:38 So still intact. 01:40 The most important or the one that you want to know as far as your ductal carcinoma in situ is a subtype known as comedocarcinoma. 01:49 If you take a look at the histologic picture, you’ll notice that here the middle of it, it’s undergone necrosis. 01:56 The central portion of your tumor has undergone necrosis, you call this comedocarcinoma.
About the Lecture
The lecture Types of Non-Invasive Breast Cancer by Carlo Raj, MD is from the course Reproductive Pathology: Breast Disease with Carlo Raj.
Included Quiz Questions
Which statement about breast ductal carcinoma in situ is CORRECT?
- It does not go through the basement membrane.
- It describes any dysplastic lesion.
- It is invasive.
- It most commonly arises from luminal hyperplasia.
- It involves liquefactive necrosis.
Author of lecture Types of Non-Invasive Breast Cancer

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very good, complete, didatic and simplyfied, i loved this lecture. thank you, Dr Raj
