Playlist
Show Playlist
Hide Playlist
Pelvis, Bladder and Urethra Injury

-
Slides AbdominalInjuries Surgery.pdf
-
Download Lecture Overview
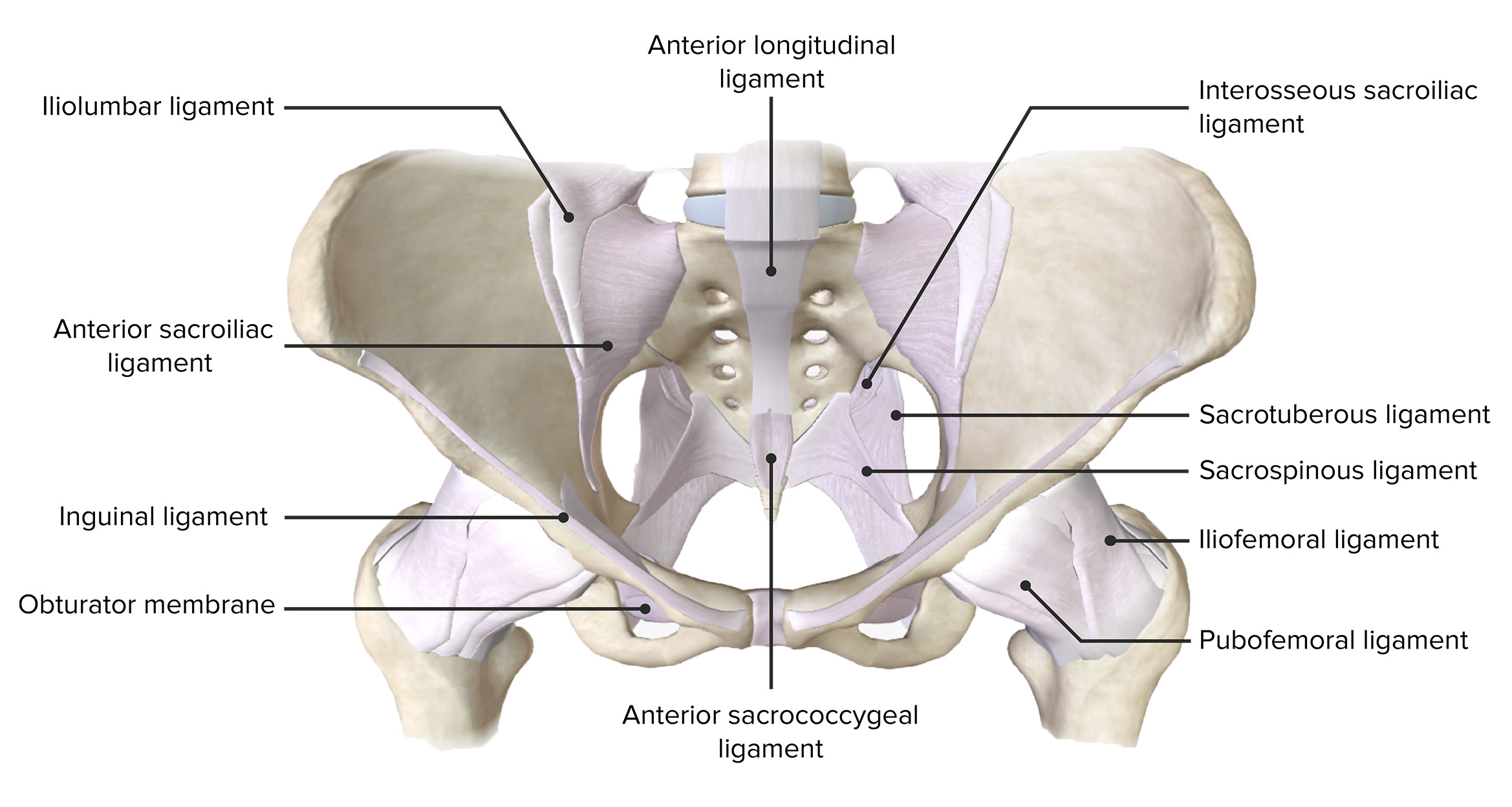
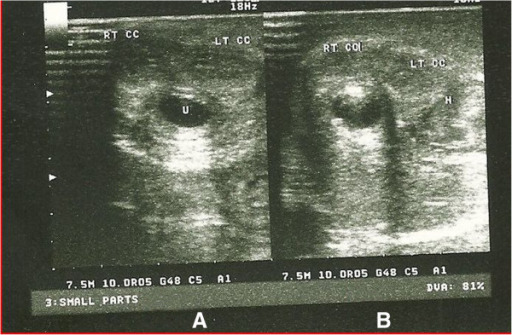
00:01 Now, let's leave the abdomen for now and go into the pelvis. 00:05 Specific pelvic injuries are – are really pelvic fracture related. 00:12 Can an eFAST detect retroperitoneal which is most likely associated with a pelvic fracture? The answer is a no and that's a major downfall of eFAST. 00:23 So just because there's no fluid peritoneum, doesn't mean that there's actually no bleeding in the retroperitoneum, that would be a miss. 00:33 Now take a look at these x-rays. This patient has a pretty bad pelvic fracture. 00:38 In fact, you see the widening of the symphysis, maybe an open book pelvic fracture. 00:43 Significant pelvic fractures like this is associated with – with retroperitoneal hematoma and bleeding. 00:49 Although in general, these are self-limited. 00:52 In a patient whose unstable, and this is an important caveat who demonstrates active extravasation. 00:59 Instead of rushing to the operating room, what we actually do is take patient into the interventional suite after put – placing a pelvic binder. 01:06 So again remember, if you have an isolated pelvic fracture and it's on an unstable patient, you wanna wrap their pelvis in a pelvic binder and then take them into the interventional suite. 01:18 This is because unlike intra-abdominal organs that are bleeding, opening up the abdomen potentially makes the bleeding worse because the previous tamponade has been released. 01:29 Here you seen an interventional angiography demonstrating extravasation. 01:34 Here our interventional radiology colleagues can do selective embolization. 01:40 And in the lower quadrant of the image, you see the fixation. 01:45 Often times particularly when the patient's hemodynamically unstable, our orthopedic colleagues will place what's called an external fixator just temporizing and stabilizing the pelvis so that no further bleeding occurs. 01:59 This also reduces the volume and space that's available in the retroperitoneal – in retroperitoneum for bleeding. 02:09 Now, what are some associated injuries with pelvic fractures? Don't forget these, these are important. That's right, bladder and urethra injuries. 02:20 Let's go over them quickly. 02:24 First, we'll take a look at bladder injuries. 02:27 In bladder injury, the most important differentiation is whether or not the bladder injury is an intraperitoneal or extra-peritoneal position. 02:36 Now, for extrapertioneal injuries as demonstrated by this contrast study, there's contrast exiting the bladder but limited itself to the extraperitoneal space. 02:47 This is an important distinction because in this situation, foley dainage alone is enough. 02:52 As oppose to an intraperitoneal bladder injury where there's free contrast flowing or urine flowing intra-abdominally, this usually requires surgery to repair the bladder multiple layers. 03:06 Now remember pelvic fractures are also associated with urethral injuries. 03:11 What are some classic exam findings of a urethral injury? Well, high riding prostate and blood at the meatus. 03:18 In fact, if you take ATLS or Advance Trauma Life Support Systems, these are – these are important clinical findings that we record at every trauma activation. 03:30 If there's suspicion of a urethral injury prior to placing a Foley catheter, you must perform a urethrogram. 03:38 This is generally – either done under fluoroscopy or under CT where contrast is placed at the tip of the penis angles retrograde into the bladder. 03:48 And in disruption of the urethra needs to be handled by an urologist. 03:52 Although often times, you'll the urologist simply place a stented Foley across the urethral injury obviously very carefully. 04:01 Urethral injuries are also associated with bladder injuries. 04:03 That's why it's not good enough just to look at the urethra, we should also look at the bladder. 04:08 Now it's time to review some very important clinical pearls and high-yield information. 04:13 First, don't take an unstable patient to the CAT scanner, it's a disaster ready to happen. 04:18 And remember, in a clinical scenario presented to you where the patient becomes hemodynamically unstable, requires immediate intervention, no further diagnostic studies. 04:29 We can either go to interventional radiology for example in a patient has a pelvic fracture or the vast majority of the time, they need an exploratory laparotomy. 04:38 And I strongly recommend that that's the choice you pick on your examinations. 04:44 Thank you very much for joining me on this discussion of abdominal and pelvic injuries.
About the Lecture
The lecture Pelvis, Bladder and Urethra Injury by Kevin Pei, MD is from the course Surgery: Trauma. It contains the following chapters:
- Pelvis
- Pelvic Fracture
- Bladder and Urethra Injury
Included Quiz Questions
Which of the following are associated with pelvic fractures?
- Bladder and urethral injury
- Colon injury
- Kidney injury
- Rectal injury
- Abdominal injury
An examination revealing a high riding prostate and blood at the meatus are indications of which of the following?
- Urethral injury
- Colon injury
- Bladder injury
- Rectal injury
- Kidney trauma
A trauma patient presents in the trauma bay with hypotension, tachycardia, and altered mental status. After completing your ABCs, what is your next step?
- Intravenous fluid therapy
- Interventional radiology
- MRI
- CT scan
- Antibiotics
Author of lecture Pelvis, Bladder and Urethra Injury

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
