Playlist
Show Playlist
Hide Playlist
Toxoplasmic Meningitis

-
Slides Other CNS Infections.pdf
-
Download Lecture Overview
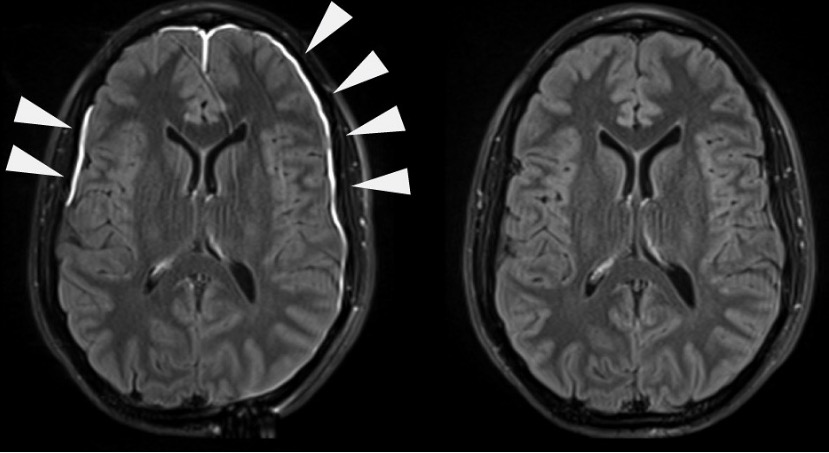
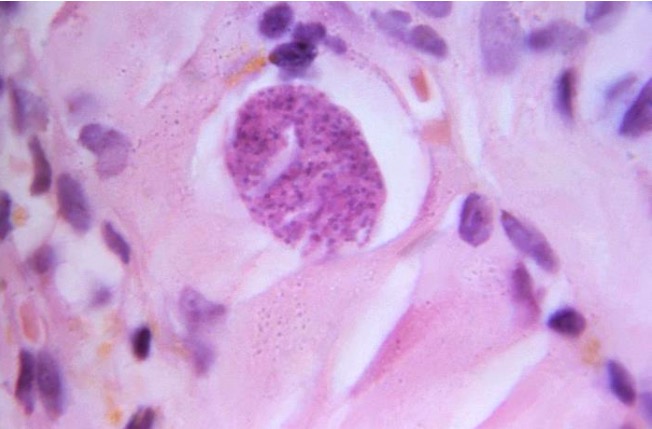
00:00 Now let's move to toxoplasmosis or toxoplasmosis meningitis. Toxoplasmosis is a common complication of AIDS and can be seen in HIV AIDS patients whose CD4 count has dropped to less than 200 or 100. Toxo is one of these interesting infections that's thought to be a reactivation syndrome. This is a parasite that can live within us and our immune system normally keeps at bay until the immune system is suppressed. And again, when CD4 counts drop, the immune system is unable to survey the body and prevent toxoplasmosis reactivation and we see reactivation anywhere in the body but there is a predilection or a tropism for the brain and specifically for the basal ganglia. Patients present typically like a cerebritis or brain abscess. We see fever, headache, and a focal neurologic deficit with or without seizure. 00:58 That should point us to cerebritis or a brain abscess, that type of CNS infection and we need to get imaging to evaluate those patients. The diagnosis is typically based on imaging and MRI is the most sensitive and specific method for evaluating these patients, and they are treated with sulfadiazine and pyrimethamine with or without leucovorin and often for a prolonged course to eradicate the entirety of this infection. In HIV positive patients, toxoplasmosis prophylaxis preventing the development of this reactivation is critical for patients whose CD4 counts are low and typically we would think of prophylaxing with antibiotics when CD4 counts have dropped below 200 or certainly 100. The typical prophylaxis is Bactrim or trimethoprim-sulfamethoxazole which is given daily or 3 times a week as a prophylaxis agent for patients whose CD4 counts are less than, again, about 200. What do we see with imaging? Because imaging is really the mechanism of choice for evaluating these patients, well here we see a T1 gadolinium enhanced image and we see an abscess, we see a lesion in the right frontal lobe that enhances avidly with contrast. It is a complete ring of enhancement. Again, enhancement is seen, gadolinium enhancement is seen with acute infections, inflammation, and malignancy. Inflammatory lesions often cause an incomplete ring of enhancement which we don't see here, this is a complete ring, and when we differentiate infections from malignancy we're looking at central restricted diffusion and lesions that show prominent restricted diffusion are favored to be abscesses over a malignant cancer. We can also see that on this post-mortem assessment, we see this area of a prominent lesion with surrounding edema and often the edema around these lesions is substantial. This causes increased intracranial pressure, mass effect, sometimes midline shift, and can become very problematic for patients if not recognized and treated quickly.
About the Lecture
The lecture Toxoplasmic Meningitis by Roy Strowd, MD is from the course CNS Infections.
Included Quiz Questions
What is the preferred modality of diagnosis for toxoplasmosis meningoencephalitis?
- Magnetic resonance imaging (MRI)
- India ink preparation of the CSF
- Toxoplasma IgG immunoglobulin in the serum
- Lymphocyte CD4 count of the CSF
- P24 antigen test in the serum
What is the drug of choice for prophylaxis against toxoplasmosis in HIV patients?
- Trimethoprim-sulfamethoxazole
- Sulfadiazine and pyrimethamine
- Rifampin
- Acyclovir
- Benzathine penicillin G
Author of lecture Toxoplasmic Meningitis

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
