Playlist
Show Playlist
Hide Playlist
Lymphadenopathy: Thymoma – White Blood Cell Pathology

-
Slides Lymphoid Tissue Thymus White Blood Cell Pathology.pdf
-
Download Lecture Overview
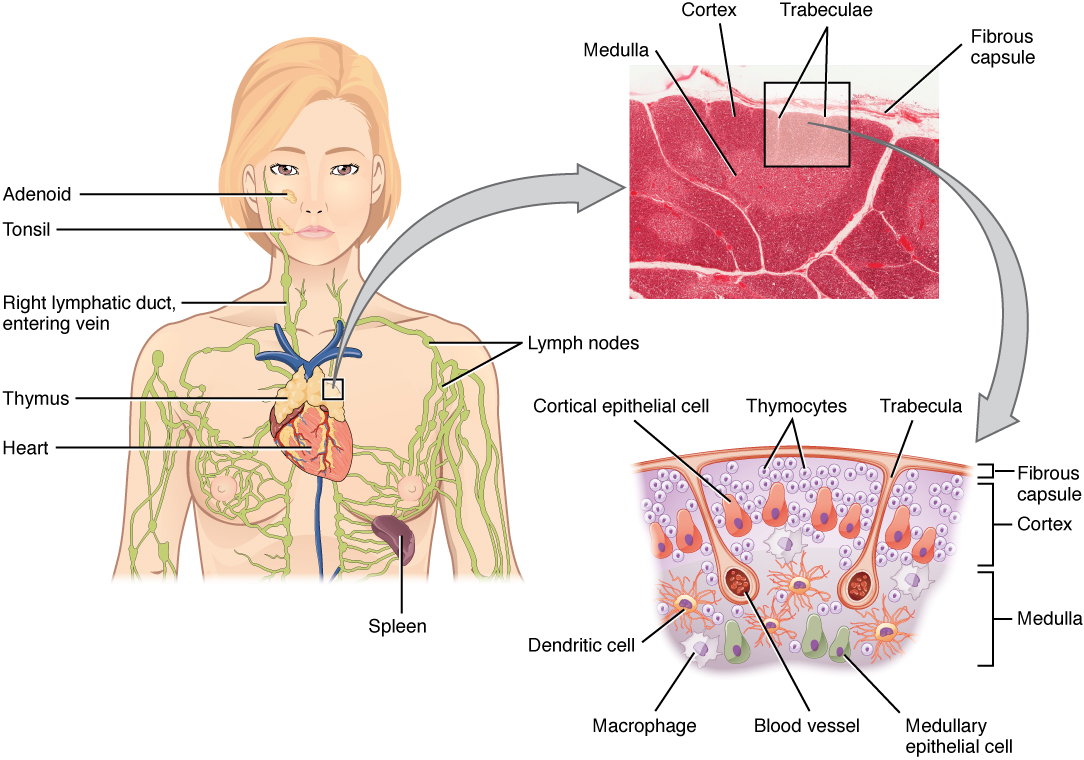
00:02 Thymomas. 00:03 A tumor of thymic epithelial cells perhaps. 00:07 Admixed non-neoplastic lymphoid cells maybe present. 00:11 Easily confused with a lymphoma because you’re not expecting to find a large thymus in an adult perhaps. 00:20 Stages: I, encapsulated. 00:23 II, microscopic, only locally invasive. 00:27 You get into stage III, now, we have issues. 00:31 Pay attention here. 00:33 Let’s say that thymus is undergoing enlargement due to, well, a thymoma, maybe a tumor. 00:40 Think about the surrounding structures of the thymus in the mediastinum, and you might start invading into the pericardium, great vessels or perhaps even the lung. 00:50 Of all the stages with thymoma, you focus upon stage III, please. 00:55 Stage IV will be the same basically in any type of cancer where it then goes onto metastasis. 01:03 In this table for staging or histological description of the thymomas, there are different types. 01:10 A little bit more detail than what’s necessary for you but you might get an idea as to what you can expect, especially the last column where it says disease-free survival at 10 years. 01:20 That’s what you’re paying attention to. 01:23 A, AB, 83, 83. 01:27 Now, this is where you want to pay attention to. 01:29 As you go from B2 to B3, is where you’ve dropped from 83 to 35, that is significant. 01:39 There’s a theme here or concept that you need to take away from medicine. 01:43 Anytime that you’re dealing with any cancer, I can only give you so many angles. 01:48 And from the feedback that I’ve gotten, it’s the fact that ultimately, it’s where you’re looking at prognosis where it’s decent to perhaps even good and it drops dramatically. 02:00 Those are the staging types that you want to pay attention to. 02:03 B2 to B3, you’re not going into carcinoma, you’ve dropped down to 35. 02:09 And as you go into C, well, further thymic carcinoma. 02:17 Now, when there is thymoma on chest x-ray in an adult, so let’s say that you have a female and she says, “Hey, doc. I wake up in the morning and I’m feeling fantastic. 02:29 And by the time the day is coming to an end, well, the first thing that happens is just every single day, I just have a hard time looking at the computer and I feel like I can’t even open up my eyelids. 02:43 And really, by four or five o’clock, forget about it, I can barely even get out of my chair. 02:49 On chest x-ray, you’ll find an enlargement in the mediastinum. 02:55 So therefore, this will be a thymoma. 02:57 Surgically, oftentimes, this thymoma in adult, why did I give you a female? And what kind of symptoms is she exhibiting, and most likely my diagnosis would be? Okay. 03:09 So she has myasthenia gravis. 03:11 She felt great when she woke up. 03:13 Her eyelids at first were affected because eyelids are what’s known as your type 2 muscle fibers, fast-twitch, and those are the ones that are affected first. 03:24 And then eventually, all the other muscles will be affected to the point where everything gets fatigued. 03:30 That’s because type 2 hypersensitivity, myasthenia gravis, destroying the acetylcholine receptors. 03:38 Keep in mind that if you were to remove the thymus in this patient, of the lady, then you might be seeing on chest x-ray a thymic shadow. 03:47 So either will give you a thymoma or that’ll give you a thymic shadow. 03:54 Clinical features: Acquired hypogammaglobulinemia. 03:58 In other words, what’s happening here is the fact that with thymoma, it will then have decreased proper immunoglobulin or decreased immune status. 04:09 Oftentimes, with thymoma, almost always associated with autoimmune disorders. 04:15 I discussed one with you, which was myasthenia gravis. 04:18 Is that the only one? No. 04:20 But a common one, yes. 04:23 But autoimmune diseases should come into mind or should be highly suspected if you’re finding an adult who has a thymus that’s enlarged. 04:30 Remember, we’re dealing with the thymus here. 04:33 The autoimmune disorders that you’re paying attention to, myasthenia gravis. 04:37 We’ve talked about this in immunology. 04:39 Just to make sure we’re clear, a type II hypersensivity, but this time, we’re destroying the acetylcholine receptors at the neuromuscular junction. 04:48 So therefore, what’s actually happening is the fact that, remember, you have a test called edrophonium or the Tensilon test, using edrophonium, a short-acting acetylcholinesterase inhibitor. 04:59 And therefore, upon such administration, you’d find improvement of her skeletal muscle. 05:06 Another autoimmune disorder called Good’s syndrome, which is going to be a thymoma plus a combined immunodeficiency and hypergammaglobunemia, Good’s syndrome. 05:18 Or with a thymoma, another autoimmune disorder you might be thinking about is called complete, complete absence of an RBC or the RBC population is severely compromised. 05:31 This is called pure red cell aplasia. 05:35 That means that the platelets are unaffected and also, you would have unaffected WBCs, but the RBCs will be purely affected. 05:43 Thymomas, autoimmune associations. 05:47 Myasthenia, Good’s, pure red cell aplasia. 05:51 Others: You’ve heard of Grave’s, pernicious anemia, dermatomyositis, and Cushing’s syndrome. 05:59 It could also be associated but they would give you other signs and symptoms, obviously, in which you would know quickly that you have Grave’s and pernicious anemia, B12, and megaloblastic anemia, increased risk of cancer. 06:11 You know about your pH in your stomach being increased, all the things we’ve talked about in hematology. 06:17 Dermatomyositis, you’re paying attention to the first manifestation, which would be the skin, derm, then followed by the skeletal muscle, also associated with thymomas, and Cushing’s perhaps. 06:29 Autoimmune.
About the Lecture
The lecture Lymphadenopathy: Thymoma – White Blood Cell Pathology by Carlo Raj, MD is from the course Lymphadenopathy – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following is most often confused with thymoma?
- Lymphoma
- Acute myeloid leukemia
- Chronic myeloid leukemia
- Acute lymphoblastic leukemia
- Hairy cell leukemia
Which of the following types of thymoma develops thymic carcinoma?
- Type C
- Type A
- Type B1
- Type AB
Which of the following types of thymoma develops cortical thymoma?
- Type B2
- Type C
- Type AB
- Type B3
- Type A
Which of the following neuromuscular disorders are frequently associated with thymomas?
- Myasthenia gravis
- Peripheral neuropathy
- Duchenne muscular dystrophy
- Amyotrophic lateral sclerosis
- Polymyositis
Author of lecture Lymphadenopathy: Thymoma – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
