Playlist
Show Playlist
Hide Playlist
Tension Pneumothorax, Rib Fractures and Pulmonary Contusion

-
Slides ThoracicInjuries Surgery.pdf
-
Download Lecture Overview
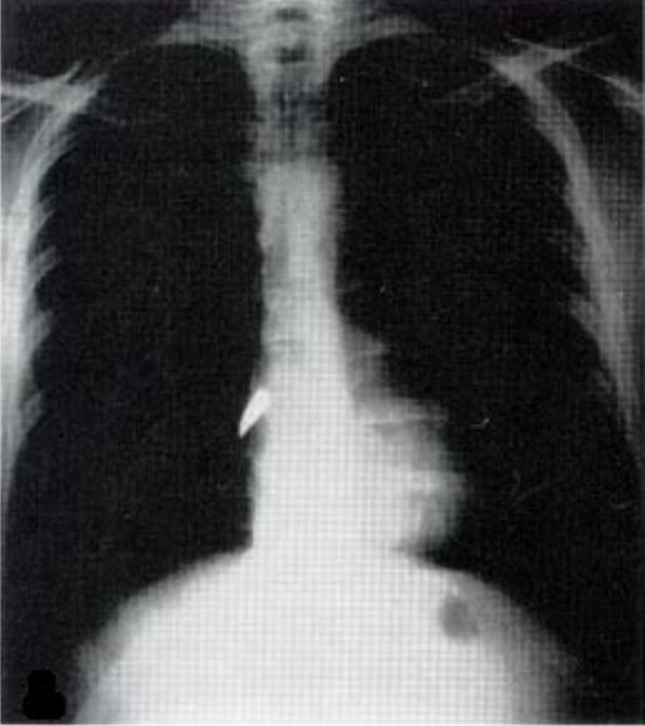
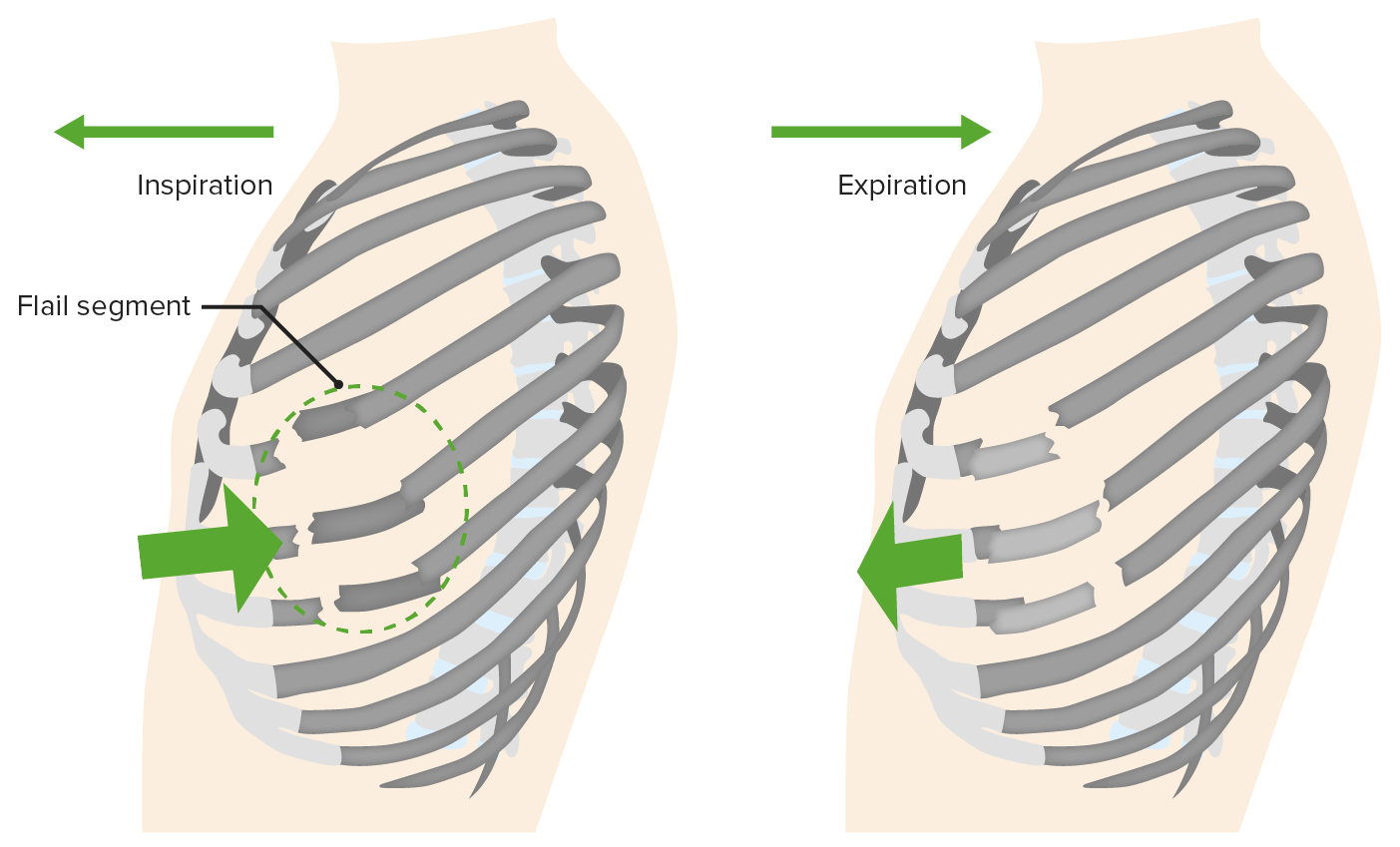
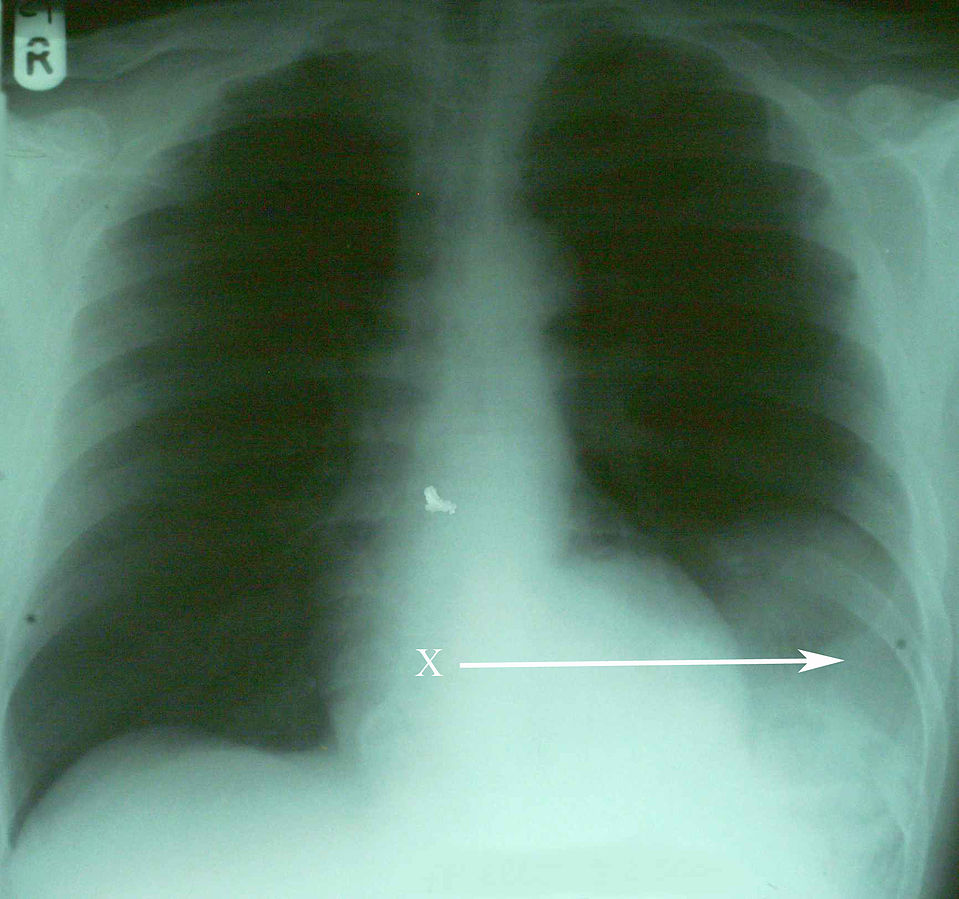
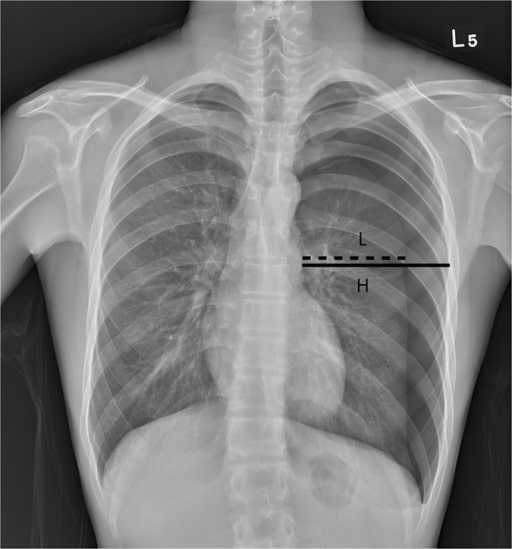
00:01 Now, what if the patient becomes hypotensive with distended jugular veins while you’re assessing the airway? What’s going on in your mind? What’s your next management step? I’ll give you a second to think about this. 00:17 That’s right. 00:19 You’re thinking the patient may have a tension pneumothorax. 00:22 Can you see what the tension pneumothorax is on this image? I’ll give you a second to look at it and then I’ll point it out to you. 00:30 You clearly see the pneumothorax in the left side, but what defines it as tension is the fact that the mediastinum has now shifted to the right side of the screen. 00:40 However, remember, tension pneumothorax should never be a radiographic diagnosis. 00:46 Remember, tension pneumothorax is a clinical diagnosis not a radiographic one and patients with tension pneumothorax or a pneumothorax associated with hemodynamic instability is at high risk for rapid deterioration. 01:00 Your quick action can save the patient’s life. 01:03 This is high-yield information. 01:07 Now, it’s important to understand pathophysiology behind tension pneumothorax. 01:12 As you know, none of our organ systems worked in a vacuum. 01:16 The interaction between the lung and the heart is very, very important. 01:21 Let’s quickly review. 01:24 In a tension pneumothorax, the pneumothorax shifts the mediastinum. 01:29 Subsequently, the pneumothorax is increasing the intrathoracic pressure. 01:34 While it’s not a very high pressure relative to baseline, it’s a positive pressure. 01:40 As a result, there’s decreased venous return. 01:43 The high intrathoracic pressure decreases the venous return. 01:48 And subsequently, there’s less filling of the heart and hypotension ensues. 01:53 This is a series of pathophysiology behind why the patients become hemodynamically unstable. 01:59 If you have a patient with absent breath sounds and presented with hemodynamic instability, the next step in management is absolutely to put a chest tube in, not to get a chest x-ray. 02:10 As a reminder, high-yield information, the decreased venous return is due to intrathoracic hypertension which leads to decreased cardiac output and hypotension and the treatment is immediate decompression with a chest tube or needle decompression. 02:26 Now let’s move on to a different topic. 02:29 Multiple rib fractures. 02:31 If you have a high velocity mechanism that causes rib fractures like it’s demonstrated on this 3D reconstruction, what’s going on in your mind? What would you like to do for the patient? And what are you concerned about? Historically, patients with multiple rib fractures particularly those with flail segments were rendered immobilize to the chest wall thinking that the chest wall immobilization would help the patient. 02:56 And the rationale behind that was patients experience significant amount of pain with the multiple rib fractures and they splinted and did not take deep breaths as a result of the pain. 03:08 Clinicians back then thought, “Well if they’re splinting because of the pain, let’s immobilize the chest wall so there’s not so much motion and decrease pain.” Unfortunately, stabilization by weights did not help. 03:20 In fact, it made things worse. 03:22 It caused atelectasis and led to pneumonia. 03:28 So, what’s the modern management? Well, largely we want to maintain pain control. 03:33 Pain control is incredibly important and there are multifaceted ways that we can control pain. 03:38 The reason we want to make sure the patient has adequate control of the pain is because we don’t want them to splint and we want them to have adequate inspiratory effort. 03:46 You can give the patient schedule narcotic pain medications as well as non-steroidals. 03:51 And sometimes, it’s helpful to place an epidural or a paravertebral block particularly in patients with multiple rib fractures or flail segments. 04:01 And so simple but very, very important and effective is pulmonary toilet. 04:06 Here, you see an incentive spirometer. 04:08 Every hospital has it. 04:10 In fact, all your patients who will get admitted should be offered an incentive spirometer. 04:15 Patients take nice deep inspiratory effort to float the balloon. 04:19 This is a similar mechanism. 04:21 Just as a reminder to you, flail segments are multiple rib fractures in multiple segments and can lead to paradoxical motion of the chest wall. 04:32 Now, what’s the big deal behind rib fractures? Well, we used to think the rib fractures in and of themselves were the problem. 04:39 In fact, the rib fractures did cause pain, but it’s actually the pulmonary contusion or bruising of the lung underneath the rib fracture that cause more problems. 04:49 Here, you see on the right side a haziness to the lung as opposed to the normal aeration on the left. 04:55 With the appropriate clinical context, for example multiple rib fractures on the right side, this is likely pulmonary contusion or bruising of the lung. 05:05 Pulmonary contusion on cross-sectional imaging is very difficult to differentiate from, for example, atelectasis or consolidation like pneumonia. 05:13 So again, clinical context is important. 05:16 Remember, what happens if you bang your knee? Swelling happens or bruising happens. 05:21 This is exactly what happens in the lung.
About the Lecture
The lecture Tension Pneumothorax, Rib Fractures and Pulmonary Contusion by Kevin Pei, MD is from the course Surgery: Trauma. It contains the following chapters:
- Tension Pneumothorax
- Rib Fractures
- Pulmonary Contusion
Included Quiz Questions
What is the first step in management after a diagnosis of tension pneumothorax is made?
- Emergent needle decompression
- Bullectomy
- Watchful waiting with supplemental oxygen
- Intubation
- Watchful waiting without supplemental oxygen
Which of the following most commonly leads to further complications as a result of rib fractures?
- Pulmonary contusion
- Atelectasis
- Dyspnea
- Rib fracture itself
- Consolidation
Author of lecture Tension Pneumothorax, Rib Fractures and Pulmonary Contusion

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
