Playlist
Show Playlist
Hide Playlist
Tachycardia: Atrial Flutter


-
Slides Tachyarrhythmia Atrial Fibrilation Cardiovascular Pathology.pdf
-
Download Lecture Overview
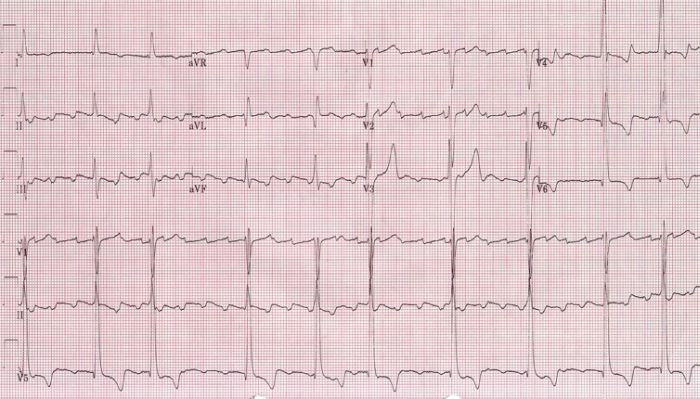
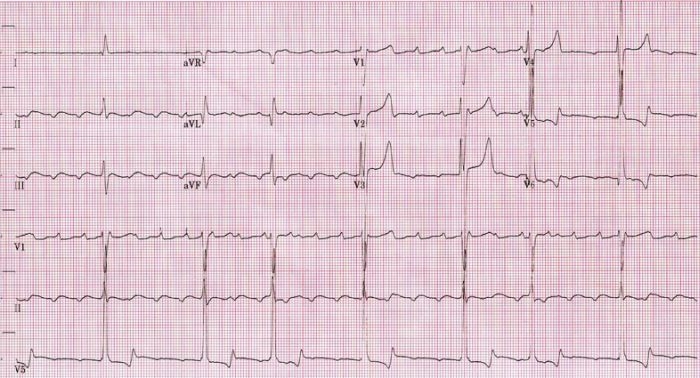
00:01 Now we already completed discussion of atrial fibrillation. Stop, take a breath, moving onto flutter. Okay. So the end part of this section for supraventricular tachycardia will end with flutter as being our discussion. Atrial flutter is a regular atrial tachy. 00:22 Read regular. What happened to atrial fibrillation? Irregular. Next. Atrial discharge, extremely quick but you know what, we also found that with atrial fibrillation, but interestingly enough you want to take a look at the following. 300 beats per minute shall we say, then 2:1 fashion in terms of its ratio. What does that mean? A 2:1 to P waves to every QRS complex, leading to a regular tachy at approximately 100 beats per minute. So for every QRS complex that you get, you might have two P waves giving you a total of how many? 250 to 300 beats per minute as far as atrial conduction, but then in terms of its regular tachy, it will approximately 150. Makes sense of that? That is your simple math. 01:11 Now the "F-waves" on ECG will then give you your sawtooth. Let me take a look at this ECG. Sawtooth type of appearance, regular rhythm, the QRS complex is showing up regularly and it is a fact that it is a 2:1 ratio. So look for that and you will be in good shape for flutter. Well take a look at some etiology and such coming up shortly. Patient can be asymptomatic present with palpitations, lightheadedness, now syncope all these are nonspecific all because of decreased cardiac output as you can imagine. Palpitations, increase heart rate, lightheadedness, and syncope. Causes. Now I'm going to slow down here just a little bit. 01:49 Make sure that we are clear. The causes that we saw for atrial fibrillation were very common things such as hypertension, diabetes mellitus, pulmonary embolus, so on and so forth. 02:00 Here with atrial flutter, a little bit different. Post-bypass, huge. We have PE in both, atrial fibrillation, atrial flutter. Irregular, what does that mean to you? Afib. Regular, you're thinking about atrial flutter. Valvular heart disease, CHF and perhaps even digitalis or digoxin toxicity. Causes of atrial flutter. You really want to pay attention to that ECG. Sawtooth is what we saw and we'll talk about rate control. Once again here is my dig, why? Not because of its effect on inhibition of sodium-potassium pump per se, it is the fact that it is able to slow down the AV node. Which calcium-channel blocker works better on the heart? The verapamil, V verapamil, V ventricles okay. Where does it favours your dihydropyridine such as nifedipine works much more on your blood vessels. Clear? Metoprolol, what is that? A Beta-blocker. What are we trying to do? Control our rate. If there is no spontaneous cardioversion after medical therapy, then electrical cardioversion can be performed. So keep that in mind as far as the next step of management. Medically speaking you are cardioverted by using medicine, maybe dig, maybe a beta-blocker. But if that did not work, then you have to resolve to electrical cardioversion, if greater than 48 hours, 3 to 4 weeks of anticoagulation. Now, what are you seeing here? Take a look at the bottom strip and you find that you have atrial flutter here. Keep in mind if you want to compare this to atrial fibrillation, please. This is going to be a 2:1 type of flutter, which means that you will have an atrial conduction of approximately 200 to 300 beats per minute, with the QRS complex of 150. 2:1. Now, what are you seeing there is the fact that the atrial flutter was a sawtooth type of appearance.
About the Lecture
The lecture Tachycardia: Atrial Flutter by Carlo Raj, MD is from the course Arrhythmias: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is TRUE for both atrial flutter and atrial fibrillation?
- They both may present with palpitations.
- They both have irregularly irregular rhythms.
- Neither is related to valvular heart disease.
- Only atrial fibrillation requires rate control.
- They both involve 2:1 block.
Which of the following medications is a nondihydropyridine calcium channel blocker?
- Verapamil
- Nifedipine
- Propanolol
- Amlodipine
- Metoprolol
Author of lecture Tachycardia: Atrial Flutter

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
