Playlist
Show Playlist
Hide Playlist
Substance Abuse in Adolescents

-
Slides SubstanceAbuse Pediatrics.pdf
-
Download Lecture Overview
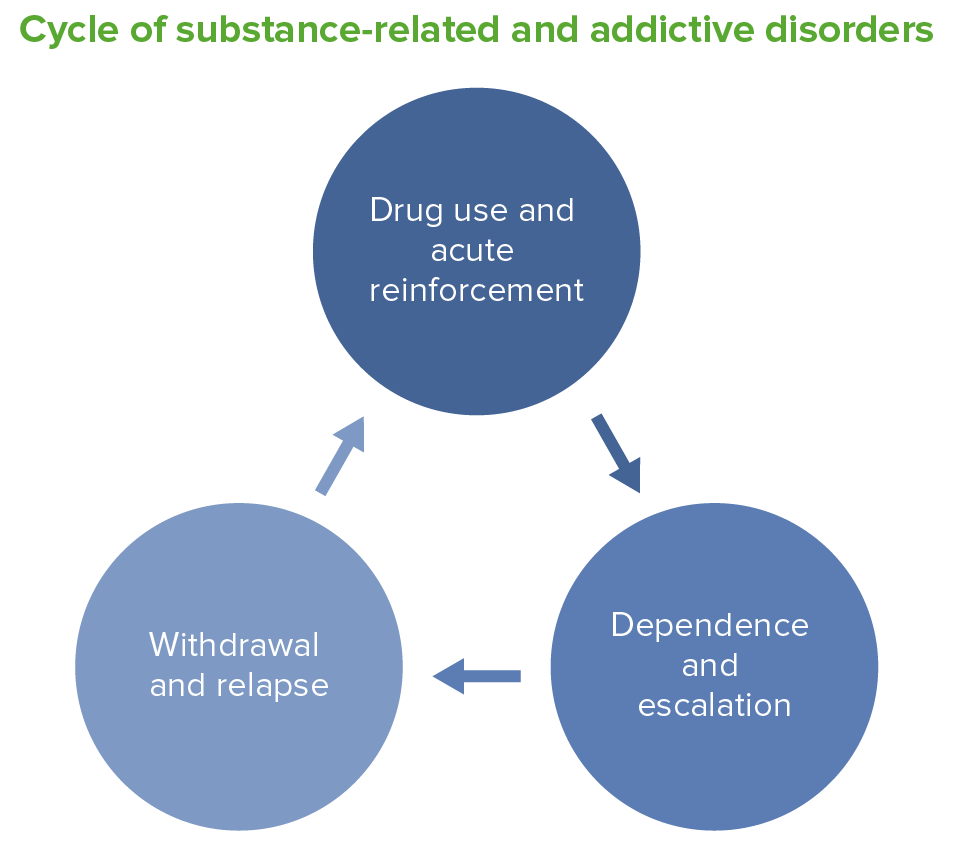
00:01 In this lecture, we will review the basics of substance abuse in adolescents. This is a huge topic and we could never do it justice but we’ll cover the important areas. So, substance abuse is a very prevalent problem in the United States. In substance abuse, we would define it as the use of a drug which results in physical, psychological, financial, legal, or social distress. 00:29 In other words, it’s not substance use. It’s substance abuse. Substance dependence is when there is substance abuse accompanied by tolerance withdrawal, unsuccessful efforts to stop, or continued abuse despite awareness of having persistent problems related to that use. So, this is how we can distinguish a child who’s for example abusing or dependent on a drug versus one who is experimenting. 00:59 Alcohol, tobacco, and marijuana are the most commonly used substances by adolescents in the US. 01:06 Roughly 1/3 of all 10th graders report the use of illicit drugs in the last year. Comorbid mental health conditions are common among those who use substances. Adolescent development and drug use is intertwined in many ways. Sometimes adolescents are more likely to use drugs because they in particular can fail to recognize long term consequences of drug use. There is a lot of primary peer influence and need for acceptance among adolescents which may drive increased likelihood of use. 01:44 Adolescents may struggle with autonomy or challenge of parental authority. They’re dealing with becoming themselves and becoming their own person and relieving themselves of parental authority and they’re making that transition. The drugs may make things feel transiently better, although in the end, there may be long term consequences. In adolescents, sometimes we under recognize the role of depression and mental health problems. Those can feel better transiently with drug use which drives up use and abuse of these drugs. Also, adolescents naturally are in a stage in their lives when they’re interested in experimenting, when they’re interested in taking risks. 02:29 So, when there is a feeling like taking a drug may be a risky thing to try but intriguing, they’re more likely to do it than an adult in a similar circumstance. Causes of drug use and drug abuse are complex. 02:44 They involve genetic, neurobiologic, and social factors. Certainly, you may have a predisposition to drug abuse if it runs in your family. But that may be both genetic and environmental. 02:58 There is increased concordance of drug abuse in monozygotic twins. So, there are some risk factors environmentally though that can tip you off that a child may be at increased risk for drug abuse. 03:16 Examples would be parents or peers who use drugs, poor parental supervision, decreased impulse control in that patient. An early age of first exposure or intoxication is likely to herald a drug abuse problem. Mood or anxiety disorders commonly are associated with drug abuse. 03:37 Patients with conduct disorders or antisocial behaviors are more likely to use drugs. 03:42 When you have a patient where you want to intervene or want to find out if they’re using drugs, it’s critically important to interview the adolescent alone. The presence of a parent is really not even a screen for drug abuse. Before talking about drugs, it’s important to establish a trusting and therapeutic relationship. So, you have to set the stage for sitting down and talking to an adolescent and have them understand that you are a person who they can trust, who they can interact with and for whom information is confidential. You also should establish upfront what information will not be confidential such as if they disclose that they’re being abused or want to commit suicide. 04:28 Establish these rules upfront and therefore, you’ll engage in a trusting relationship and then you can engage and discuss about drug abuse and other more personal questions. 04:40 When you get past that setting the stage moment, it’s important to ask other questions as well. 04:46 Ask about weight loss or mood swings. Are they having problems with sleep? Do they have a decline in academic performance, school truancy, suspensions? These are all signs of drug abuse. 05:01 You can also use the CRAFT screening tool. The CRAFT screening tool is a mnemonic for things that are putting children at risk for becoming drug abusers as opposed to experimenters. 05:16 So, C stands for car. Have you ever ridden in a car driven by someone including yourself who is high or had been using alcohol or drugs? R stands for relax. Do you ever use alcohol or drugs to relax, to feel better about yourself or fit in? A is alone. Do you ever use alcohol or drugs while you are by yourself alone? F is friends. Do your family or friends ever tell you that you should cut down on your drinking or drug use? And T is trouble. Have you ever gotten in trouble while you were using drugs or alcohol? If a patient is responding yes to these questions, they're at increased risk for having a problem with the drugs as opposed to just using them experimentally. 06:03 There are also some physical exam findings that you can see as a result of drug use. 06:09 For alcohol, patients are often disinhibited, will have slurred speech, ataxia, emotional ability, and will report having blackouts where they have interacted in ways with people and have no memory of that experience. For marijuana, patients generally develop euphoria. They may have red conjunctivae, a dry mouth and throat, increased appetite, or impaired reaction time and with very frequent chronic use may develop gynecomastia. For stimulants, patients are often hyperalert, restless, agitation. 06:43 Aggression is possible. They may have paranoia. Frequently while high, they have tachycardia and hypertension. They may suffer arrhythmias. You will note dilated pupils. In severe cases, they may have seizures. Patients on opioids tend to be drowsy or euphoric. They may have flushing or a floating feeling. They may have constipation as a side effect of the medication. 07:08 They may have miosis or very small pupils. They can suffer respiratory depression and in severe cases, hypotension or overdose may result in death. For hallucinogens, patients may develop dizziness, a heightened sensual awareness, nausea, or hallucinations, or flushing, an elevated temperature, tachycardia, and mydriasis. In inhalant use, you may notice dizziness, headaches, slurred speech, sleepiness, lacrimation, rhinorrhea, mucous membrane irritation from the inhalants getting in their mouth, ataxia, or impaired memory. So, let’s review the pupillary response because I think it’s important to remember and it can be confusing. Miosis is pinpoint pupils. This is what you see in opiates. 07:58 Mydriasis in enlarged pupils. You see this typically in stimulants. The sluggish pupillary response is present in barbiturates. A rotary nystagmus which is fairly unusual is something we see specifically with PCP. You may see skin identifications which can tip you off that a patient is a drug user. 08:22 Certainly, track marks, a cellulitis, abscesses, or phlebitis are all signs of a patient who likes to inject drugs. 08:29 Patients with rhinitis, nasal septum damage, or a nasal septal perforation may be snorting drugs such as especially cocaine. Mental status changes can be seen in patients with chronic cognitive changes or acute distortions in reality. These are signs of chronic mental altering drugs. So, how do we diagnose a patient with a substance abuse problem? Certainly, screening for other mental health problems is important. We can do urine or blood drug testing. But it’s important not only just to test for drugs but for test for problems that can come along with drugs. So, HIV testing is key both in patients who are having unprotected sex because of poor decisions while high or in patients who may be sharing needles in IV drug abuse. STD testing is often indicated in patients who use drugs as under the influence of drugs were less likely to think about things like remembering to use a condom. 09:38 Testing should target a problem. We don’t necessarily just universally drug test. 09:46 Drug testing may be necessary if a patient is hospitalized or if there are legal considerations at foot. 09:54 But generally speaking, we don’t need to just do drug testing on adolescents as it may interfere with our therapeutic relationship.
About the Lecture
The lecture Substance Abuse in Adolescents by Brian Alverson, MD is from the course Adolescent Medicine. It contains the following chapters:
- Substance Abuse
- Historical Findings
- Physical Exam Findings
Included Quiz Questions
Which of the following drugs is most likely abused in a patient with decreased level of consciousness and pinpoint pupils?
- Opium
- Alcohol
- Marijuana
- Amphetamine
- Cocaine
Which of the following best describes substance dependence?
- Substance abuse despite awareness of related persistent problems
- Drug abuse leading to physical distress
- Abuse of substances causing significant social anxiety
- Intermittent substance abuse leading to profound pleasure
- Major depression caused by chronic drug abuse
Which of the following is TRUE regarding substance abuse in adolescents?
- Increased concordance is seen in monozygotic twins.
- Peer pressure is an under-recognized cause.
- Parental drug abuse decreases risk.
- History taking must initially take place in the presence of parents.
- Alcohol abuse is not regarded as substance abuse.
Which of the following is NOT a risk factor for substance abuse in adolescents?
- Increasing number of hours spent outside home
- substance abuse by peers
- Mood or anxiety disorder
- Decreased impulse control
- Conduct disorder
In the CRAFFT screening test, what does the ‘A’ stand for?
- Alone
- Avoid
- Alcohol
- Abuse
- Addiction
Which of the following drugs is typically associated with rotary nystagmus?
- Phencyclidine
- Diazepam
- Cocaine
- Alcohol
- Marijuana
Author of lecture Substance Abuse in Adolescents

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
A topic which is not often enough talked about in pediatrics. Very common, though. Thank you!
