Playlist
Show Playlist
Hide Playlist
Spinal Cord Syndromes

-
Slides SpinalCordSyndromes Surgery.pdf
-
Download Lecture Overview
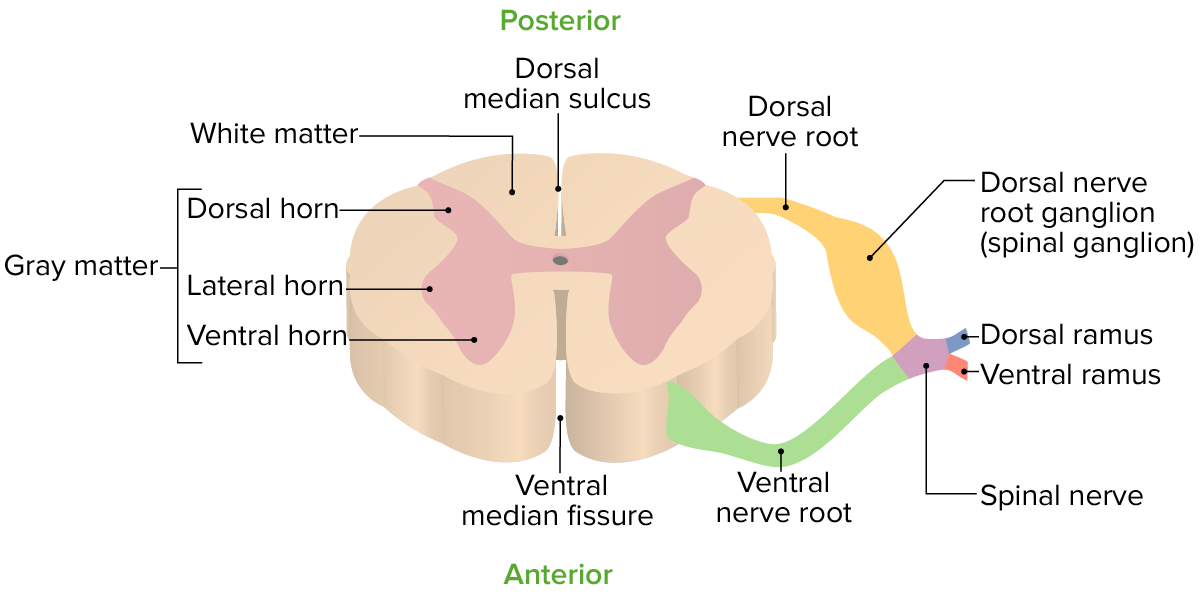
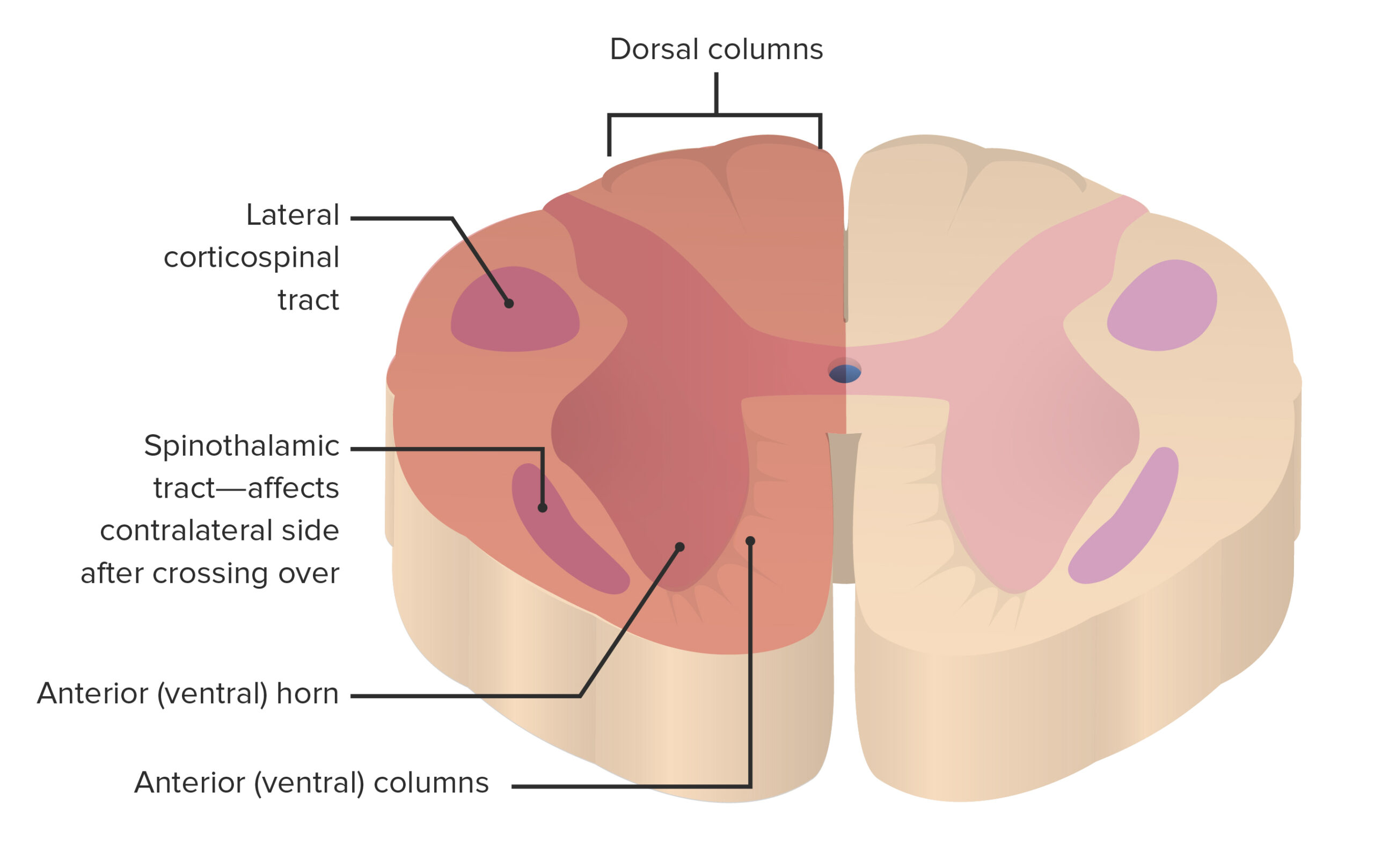
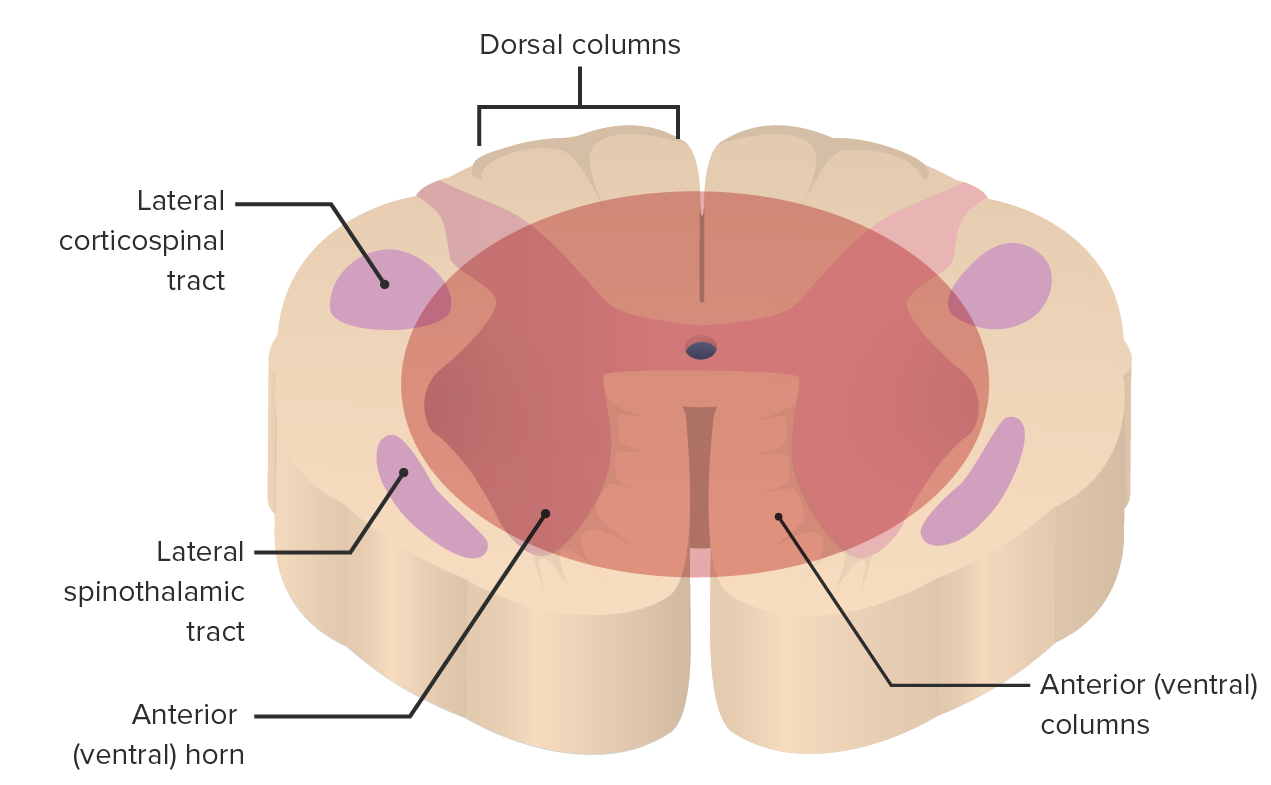
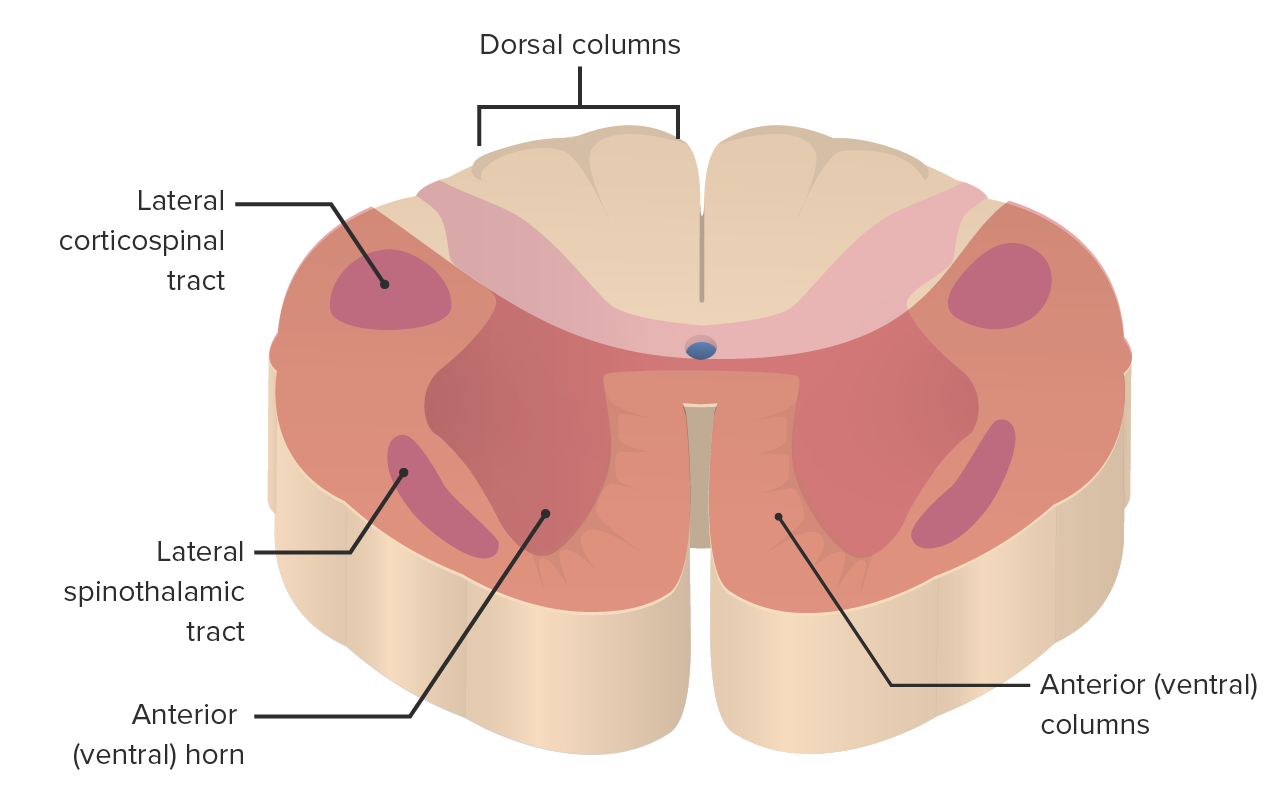
00:01 Thanks for joining me on this discussion of spinal cord syndromes in this section of neurosurgery. 00:07 Remember, spinal cord syndromes can be a little confusing, but they're incredibly high yield information for examinations. 00:13 And frankly, they're kind of fun to talk about. 00:16 Let's begin. 00:18 We can't talk about spinal cord syndromes unless we have a basic understanding of the important spinal columns. 00:24 Here. 00:25 I'll describe to you four very important spinal columns, so that you can understand when one of them is injured, what the resulting pattern would be. 00:33 The lateral and anterior cortical spinal tracts or columns are part of the pyramidal tracts and are responsible for motor function. 00:41 Next, the dorsal columns are responsible for transmitting proprioception and fine touch sensations, and lastly, the anterolateral system, including the spinal thalamic pathway, is important for transmitting pain, temperature, pressure, and crude touch sensations. 01:02 These pathways become very important, particularly when we start talking about incomplete spinal syndromes. 01:09 First, we have the Brown-Séquard syndrome. 01:12 Next we will discuss the anterior cord syndrome. 01:16 After that, we will cover the central cord syndrome. 01:20 Finally, we will examine the posterior or dorsal cord syndrome. 01:25 We're going to discuss all of these and findings that are classic for these incomplete cord syndromes. 01:31 You'll probably want to look at these slides several times to commit them to memory. 01:36 Let's begin with Brown-Séquard syndrome. 01:40 Brown-Séquard syndrome is due to a hemi-transection of the spinal cord. Due to this hemi- transaction of the spinal cord you can go back to the previous slides and figure out which of the tracks are affected. 01:53 The findings include ipsilateral, upper motor neuron paralysis and loss of proprioception, as well as contralateral loss of pain and temperature sensation. 02:01 The reason for this is because the spinal thalamic tracks cross over to the contralateral side of the spinal cord, primarily at the level of their entry. 02:11 This decussation occurs in the anterior white commissure, typically within 1 or 2 segments above the point of entry into the spinal cord. 02:20 There can also be ipsilateral lower motor neuron lesion signs at the level of the lesion due to the injury of the anterior horn cells. 02:28 The anterior cord syndrome results from injury to the anterior or ventral two thirds of the spinal cord. 02:35 The dorsal columns are spared. Clinical manifestation or loss of motor and sensory function below the level of injury. 02:43 Remember, the dorsal columns are important for proprioception and fine touch, which is preserved. 02:50 Now let's talk about central cord syndrome. 02:53 It typically occurs in elderly patients with preexisting cervical stenosis who experience a hyperextension injury. 03:00 Other causes include syringomyelia or intramedullary tumor. 03:05 The neurological exam in smaller lesions shows preferential sparing of the lower extremities and weakness in the upper extremity. 03:14 Remember, though, there are actually varying degrees of sensory loss. 03:19 It's not a very reliable exam for the central cord syndrome. 03:23 Large central cord lesions are devastating injuries with complete paralysis below the lesion. 03:29 Sacral sparing may occur. 03:32 Finally, let's examine the posterior or dorsal spinal cord syndrome. 03:38 Dorsal cord syndrome results from bilateral involvement of the dorsal columns, corticospinal tracts (CSTs), and descending central autonomic tracts to bladder control centers in the sacral cord. 03:52 The causes include neck hyperextension with atlantoaxial subluxation, tumors, the classic ”tabes dorsalis” lesion from syphilis, “subacute combined degeneration” due to B12 deficiency, Friedreich ataxia, and multiple sclerosis. 04:11 Dorsal cord syndrome commonly presents with gait ataxia and paresthesias. 04:17 Acute corticospinal tract dysfunction causes muscle flaccidity and hyporeflexia, while chronic cases result in muscle, hypertonia, and hyperreflexia. 04:29 Additionally, patients may exhibit extensor plantar responses and urinary incontinence.
About the Lecture
The lecture Spinal Cord Syndromes by Kevin Pei, MD is from the course Special Surgery. It contains the following chapters:
- Spinal Cord Syndromes
- Incomplete Cord Syndromes
Included Quiz Questions
Which of the following tracts carries pain and temperature sensation?
- Lateral spinothalamic tract
- Dorsal column medial lemniscus
- Lateral corticospinal tract
- Anterior corticospinal tract
- Pyramidal tracts
Which of the following findings are CORRECT in cases of Brown-sequard syndrome?
- Contralateral loss of pain and temperature sensation
- Ipsilateral loss of pain and temperature sensation
- Contralateral upper motor neuron paralysis
- Contralateral upper motor neuron paralysis and contralateral loss of temperature sensation
- Contralateral loss of proprioception and ipsilateral loss of pain sensation
Anterior cord syndrome leads to which of the following clinical findings?
- Loss of motor, pain, and temperature sensation at and below the lesion
- Contralateral loss of motor sensation above the level of the lesion
- Loss of deep touch and vibratory sensation below the level of the lesion
- Ipsilateral lower motor neuron paralysis
- Ipsilateral loss of pain sensations above the level of the lesion
Author of lecture Spinal Cord Syndromes

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Easy, concrete explanation, delivers what is needed without loosing the viewer during the video
