Playlist
Show Playlist
Hide Playlist
Small Bowel Obstruction

-
Slides SmallBowelObstruction Surgery.pdf
-
Download Lecture Overview
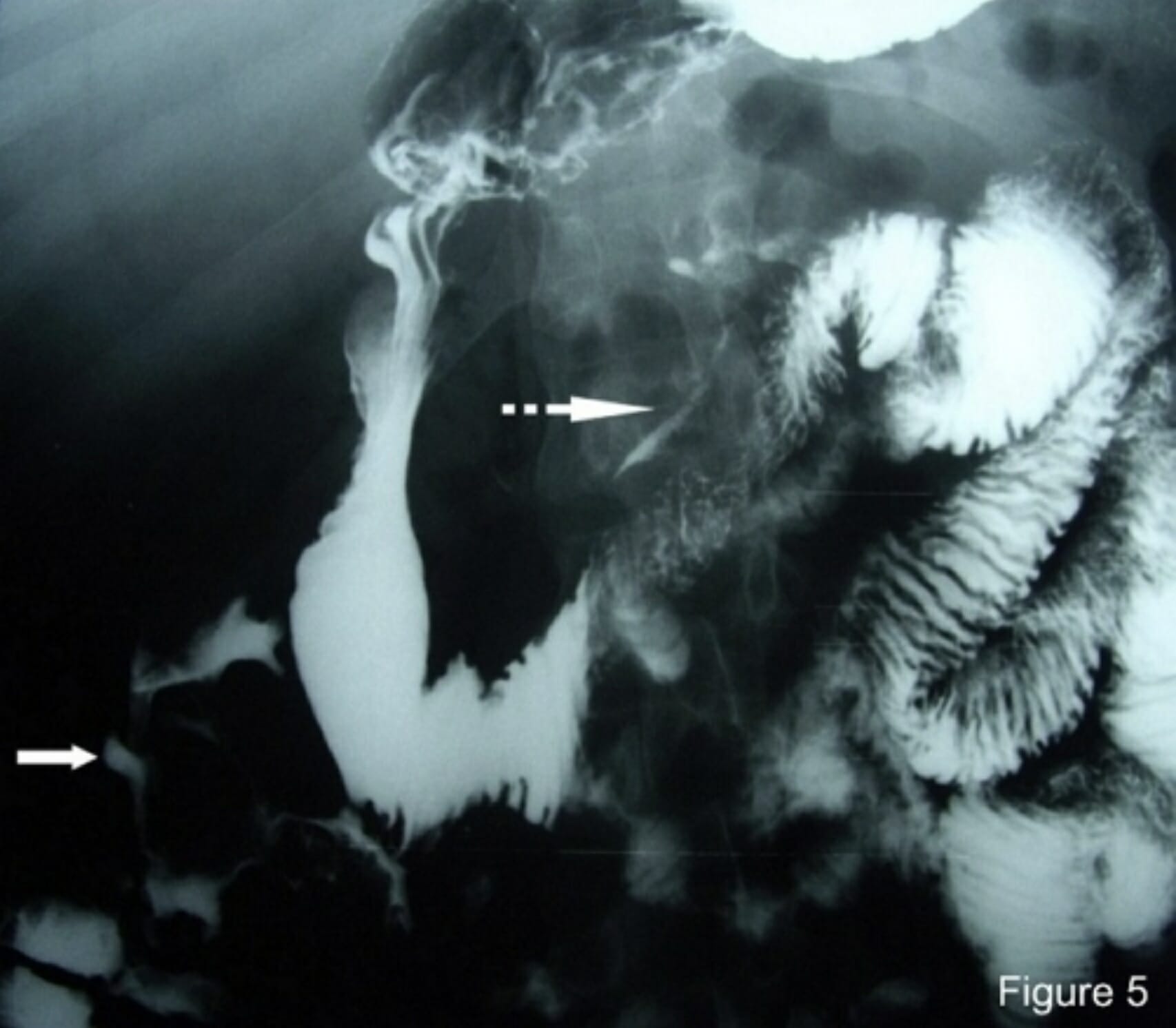
00:01 Welcome back. Thanks for joining me on this discussion of small intestines under the section of small bowel obstruction. Let’s start with a clinical case. You see a patient who is 65 years old who has a history of hysterectomy presenting to the emergency department with nausea, vomiting, and abdominal pain. 00:23 What’s on your differential diagnosis? I’ll give you a second to think about it. Of course, small bowel obstruction. It’s very high on our differential diagnosis given her previous surgery. Across the US, small bowel obstruction is a very, very common diagnosis. In fact, over 300,000 small bowel obstruction procedures were performed on an annual basis. What are the etiologies of small bowel obstructions? They include what I’ve already previously discussed, adhesions or scar tissue formed from previous surgery. 01:02 Here, you see the image of scar tissue attaching itself to the peritoneal lining. Of note, adhesions are normal body response to healing. 01:11 Virtually, all patients that undergo intraabdominally surgery develop adhesions. 01:15 Tumors can cause small bowel obstruction. Much like our discussion during the carcinoid tumor discussion, if the tumor is large enough in the small bowel, it can be a source of obstruction. Volvulus, volvulus is a twisting of the small bowel usually along the mesentery. 01:34 You’ll notice from this picture that the intestines do not look very happy. Its blood supply looks like it’s been compromised at some point. Reminder, back to the previous lectures about hernias, both groin as well as ventral hernias, in this picture you see a patient with an ostomy bag and a large loss of domain and hernia bulging from the abdominal wall. Common findings in both historical and physical findings include crampy abdominal pain, nausea and vomiting, and obstipation, again, inability to pass gas or have bowel movements. You’ll also notice that these findings are very similar to many other surgical diagnoses, which is why it’s important to have a list of high-yield differential diagnoses. 02:27 On this slide, you’ll notice that small bowel obstruction causes crampy abdominal pain. But unlike appendicitis or perforated duodenal ulcers, it’s difficult to localize to one quadrant. You’ll notice that most patients with small bowel obstructions will present with general, mild abdominal pain that’s described as crampy in nature. Clearly, this can worsen during the patient’s hospital course which may be an indication for surgery. Let’s take a look at the labs. Common chemistries: One might find decrease in the chloride; increase in the bicarb; increase in the creatinine; maybe, maybe not any changes in the white blood cell count. Though typically, unless there is intestinal ischemia or compromised bowel, the white count is typically normal. But remember, it is important to know that when you have a patient with worsening abdominal pain, increased white count or leukocytosis associated with the small bowel obstruction, one should start to begin thinking maybe the patient needs surgery sooner rather than later. 03:39 It's classic findings of nausea, vomiting in a patient, particularly one where you have placed a nasogastric tube. They’re hypovolemic because of large volume emesis and inability to tolerate PO; hypokalemia, loss of potassium through emesis; hypochloremic metabolic alkalosis with emesis due to the significant loss of chloride through stomach acids. This is important to remember as a high-yield metabolic derangement of nausea/vomiting. The kidneys try to preserve volume through the aldosterone mechanism which stimulates hydrogen and potassium excretion worsening the previous hypokalemia. Here’s the mechanism of action of aldosterone. 04:27 Commit this to memory. It’s very important. In the distal collecting tubule, you’ll notice the rectangular box simulates the tubule. In this three sodium, two potassium, one hydrogen pump, you’ll notice that aldosterone tries to hold on to the sodium while sacrificing potassium and hydrogen into the tubule which is then later excreted. This is also why patients have a paradoxical aciduria despite a metabolic alkalosis. This slide is worthwhile to review.
About the Lecture
The lecture Small Bowel Obstruction by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
Small bowel obstruction is a very common diagnosis. Which of the following is NOT a common cause of this condition?
- Infectious gastroenteritis
- Hernias
- Adhesions
- Tumors
- Volvulus
Which of the following is a typical symptom of small bowel obstruction?
- Non-localized cramping abdominal pain
- Sharp left lower quadrant pain
- High volume watery diarrhea
- Melena
- Coffee-ground emesis
A 55-year-old male patient is diagnosed with small bowel obstruction. Which of the following laboratory findings increases the likelihood that this patient will need an urgent surgical intervention?
- Elevated white blood cell count
- Elevated creatinine level
- Elevated HCO3- level
- Decreased chloride level
- Elevated red blood cell count
Which one of the following is a typical metabolic laboratory finding in a patient with small bowel obstruction?
- Hypokalemia
- Decreased HCO3-
- Hyperchloremia
- Hypervolemia
- Metabolic acidosis
Author of lecture Small Bowel Obstruction

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
