Playlist
Show Playlist
Hide Playlist
Small Bowel Obstruction (SBO) with Case

-
Slides Gastroenterology 03 Constipation.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
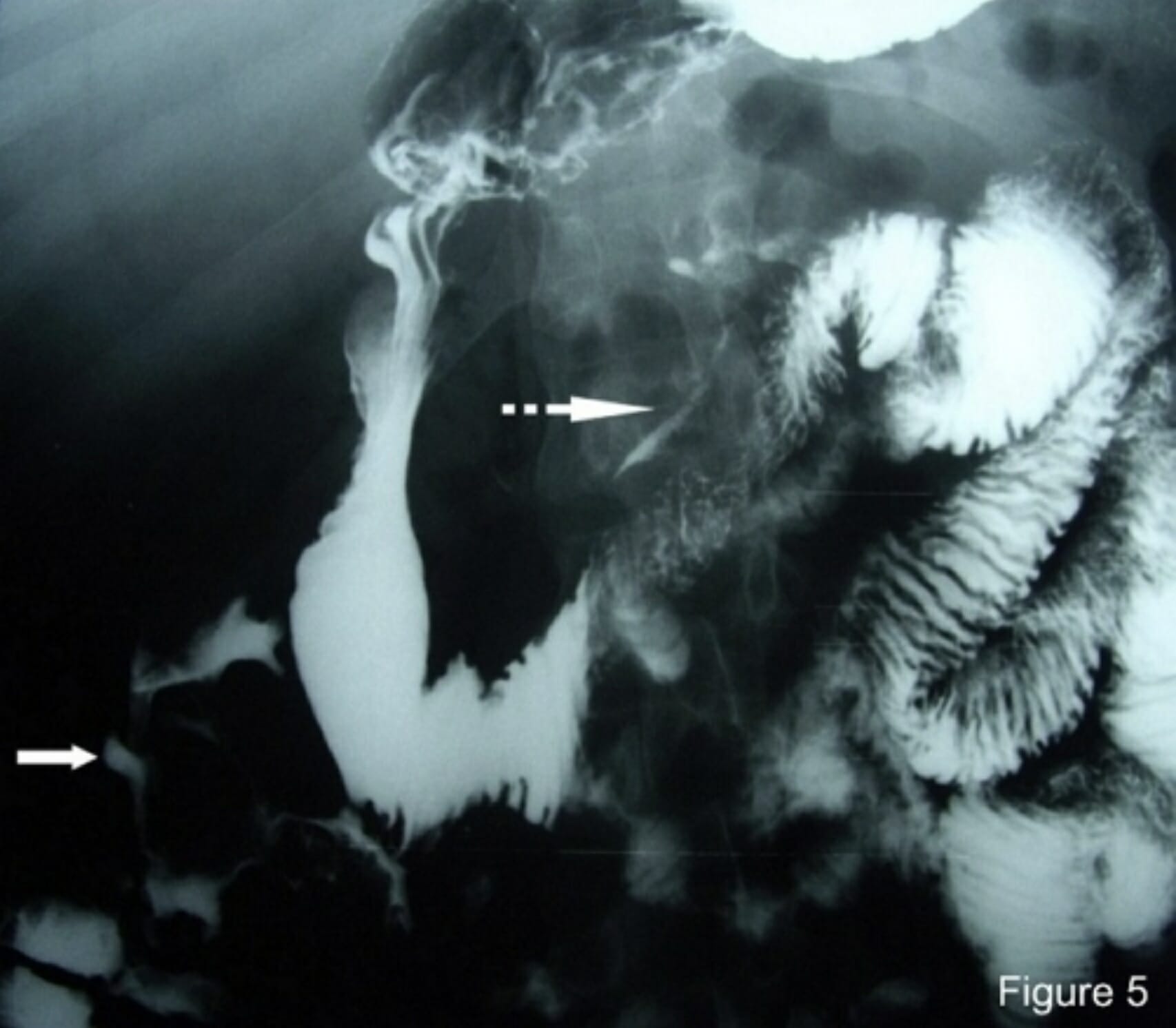
00:00 So now let's go to a case. 00:03 A 63-year old woman presents to the emergency department complaining of progressive abdominal pain, nausea and vomiting for the past 2 days. 00:12 She has not passed a bowel movement for 5 days and is not passing gas. 00:16 Her surgical history includes a prior exploratory laparotomy for a gunshot wound. 00:23 Vitals are significant for a heart rate of 110 but otherwise normal. 00:28 On exam, she has hyperactive bowel sounds, moderate tenderness to palpation and no rebound tenderness or guarding So, what is the best next diagnostic test? Let's point out some key features. 00:42 She has abdominal pain, nausea and vomiting and the absence of passing gas and bowel movements She does have a history of abdominal surgery and her physical exam is notable for hyperactive bowel sounds. 00:58 So, the first question is, what is the significance of her obstipation? Obstipation is the term we use to describe the lack of passing flatus or gas in addition to constipation. 01:13 This is a very concerning symptom for a bowel obstruction. 01:19 So, let's talk a bit about small bowel obstructions We can categorize SBO's into partial or complete obstructions. 01:28 In partial SBO's, patients are able to pass gas or have small bowel movements. 01:33 But in complete obstruction, they have complete obstipation. 01:39 Some common causes are from adhesions from prior surgeries, they may have incarcerated hernias, cancer or history of inflammatory bowel disease. 01:50 Patients will present with crampy abdominal pain, nausea or vomiting, or the presence of obstipation. 01:56 The diagnosis of a small bowel obstruction is often made by abdominal x-ray. 02:01 Computed tomography (CT) can also be used to diagnose SBO, and offers additional information such as the specific site or transition point, severity of obstruction, and whether there is an associated complication like necrosis or bowel ischemia. 02:17 So here, you could see an example of an x-ray from a patient with an SBO. 02:23 The typical features you will see are: dilated loops of small bowel, as shown here and the presence of air-fluid levels so those are horizontal cutoffs between areas of air which appears dark on the x-ray and areas of fluid which appears white on the x-ray. 02:40 The treatment of an SBO depends whether it is partial or complete. 02:44 If it is a partial obstruction, in most cases, we can treat with IV fluids, allowing for bowel rest and inserting a nasogastric tube for decompression. 02:56 If the patient has a complete obstruction, this usually requires surgery. 03:03 So now we can return to our case. 03:05 Our 63-year old woman presenting with abdominal pain, nausea, vomiting and obstipation with history of abdominal surgery and hyperactive bowel sounds. 03:14 So the important clues here are that she has acute obstipation and her hyperactive bowel sounds indicate a likely obstruction. 03:24 So now we know the best next diagnostic test is an abdominal x-ray, also known as a KUB.
About the Lecture
The lecture Small Bowel Obstruction (SBO) with Case by Kelley Chuang, MD is from the course Approach to Patients with GI Symptoms.
Included Quiz Questions
Which of the following is the treatment of choice for complete small bowel obstruction?
- Surgery
- IV fluids
- Bowel rest
- NG tube decompression
- Laxatives
Which of the following is the initial diagnostic test of choice for small bowel obstruction?
- Abdominal X-ray
- Abdominal ultrasonography
- Abdominal MRI
- Abdominal CT
- Endoscopy
Author of lecture Small Bowel Obstruction (SBO) with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
