Playlist
Show Playlist
Hide Playlist
SLE Related Kidney Disease




-
Slides KidneyDisorders RenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
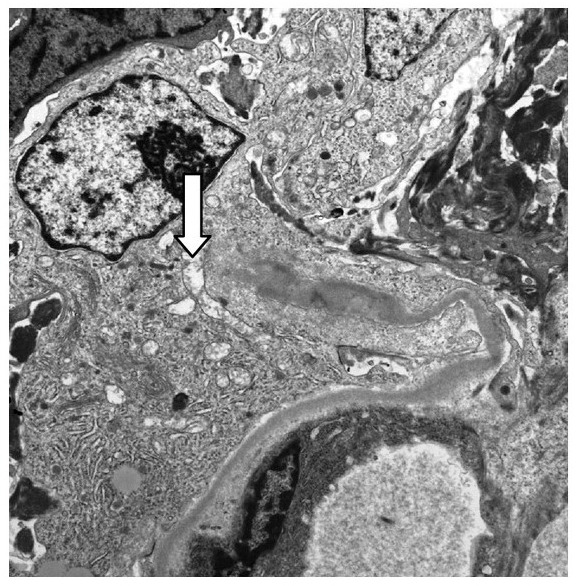
00:01 Clinical manifestation could be nephritic, nephrotic, or both. 00:04 Give me one from nephritic or give me two H and H, hypertension and hematuria. 00:11 What about nephrotic? O, massive loss of protein or it could be both. 00:15 Now, the one that you'll be paying attention as we go through this will be type IV. 00:19 So all I'm gonna do is to drop down to number four on your own time, you take a look at one, two, and three and five. 00:25 Here’s our focus. This is your focus, our focus. 00:29 The prototype under WHO classification for SLE induced kidney damage is this one. 00:37 What is it? Type IV. 00:38 How many letters in DPGN? One, two, three, four. Yes, four letters. 00:44 Type IV is DPGN. 00:45 Now, I had you memorized the D in DPGN, is what kind of deposition? Take a look at this in both sub-endothelial. Where are you? Between the endothelial cell and the basement membrane. 01:00 Are you picturing it? What kind of pattern are you going to find? A granular pattern. 01:04 This is the prototype and DPGN could be found with both nephritic and nephrotic presentation. 01:10 Now, in good faith and good conscience, there’s no way that I can move on without making sure that you do know that 10% of the time might be membranous, is that clear? So every once in a while, say that you've done your nephrology rotation, and your nephrologist was tempting you and were saying that, well, this is a patient with SLE, and define the space you're having double-stranded DNA; do not jump to conclusion and think that it’s sub-endothelial. 01:40 If you find such a patient and the deposits were sub-epithelial, then this is SLE induced kidney damage, membranous type. 01:52 If you've heard of spike and dome appearance. 01:53 Now, understand, membranous. 01:55 We haven’t even begun the discussion of nephrotic yet. 01:59 All we've done up until this point is discuss important nephritic glumerulonephritides. 02:05 We went into RPGN, even under RPGN, where did it come from? Nephritic, do you understand that? So when we touch nephrotic, guess what? I’ll repeat our membranous discussion here. 02:19 Under Type II RPGN, let’s quickly point out some Henoch-Schonlein or aka our purpura. 02:31 Take a look at the legs in our patient. 02:33 You see those areas where there looks like little red rashes? It’s not a rash, it’s actually bleeding. 02:38 Increase vascular permeability because they got damaged, the blood vessel did. 02:43 How the blood vessel could damage? If this patient, if there was a history and if I'm telling you that this child is also suffering from hematuria, chances are pretty good that if you're to do a biopsy of these lesion you would find IgA. 02:58 Welcome to IgA vasculopathy. 03:01 The reason that we have this here is because you can have IgA deposition in your kidney, and the reason that we’re talking about such vasculitis in the nephrology topic, is because of its involvement of the kidney it may result in RPGN. 03:18 Where would you find this? Arms, legs; usually lower extremity, buttocks. 03:22 Systemic childhood disorder. 03:25 By systemic we mean other organs could be involved. 03:28 IgA and IgG are the most common immunoglobulins and these will then deposit, where in the kidney? In the mesangium. 03:37 Clinical features, pain in the abdomen, vomiting, intestinal bleeding, nonmigratory arthralgia or pain but it’s the palpable purpura that you're truly paying attention to because of immune-complex deposition. 03:52 Palpable purpura. You can literally feel the purpura on this patient. 03:57 Fibrinoid necrosis is taking place in your blood vessel. 04:00 Continuing our discussion of RPGN, under type III, we’ll take a look at some of the ANCA positive, pauci-immune.
About the Lecture
The lecture SLE Related Kidney Disease by Carlo Raj, MD is from the course Glomerulonephritis.
Included Quiz Questions
Which of the following best describes the classical pathology of type IV SLE-related kidney disease?
- Subendothelial immune complex deposition and markedly thickened capillary loops ("wire loops")
- No renal involvement
- Focal proliferation
- Slight proteinuria
- Minimal hematuria
Which of the following clinical features is characteristic of Henoch-Schönlein purpura?
- Palpable purpura on the legs and buttocks
- Migratory arthralgia
- Nonpalpable purpura on the abdomen
- Dysphagia
- Dyspnea
Author of lecture SLE Related Kidney Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
