Playlist
Show Playlist
Hide Playlist
Separation of Ventricles

-
Slides 06-30 Formation of AV canals and Separation of the Ventricles.pdf
-
Reference List Embryology.pdf
-
Download Lecture Overview
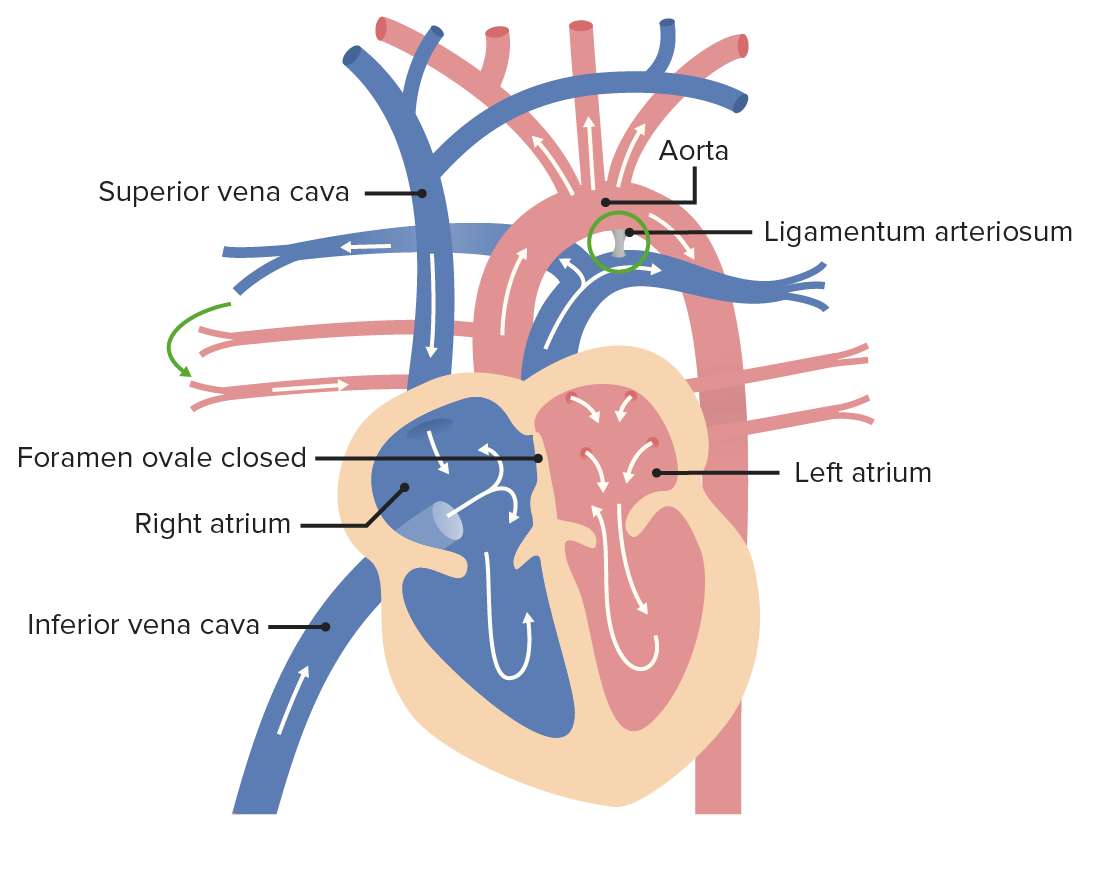
00:01 Now that's how the atrioventricular canals close. 00:04 Let's look at the closely related topic of ventricular separation. 00:09 From here, we've got a single chambered heart with the atria starting to separate, we have the septum primum growing down. 00:17 We can see a little bit of those endocardial cushions starting to pinch the atrium and ventricle away from each other. 00:24 As development proceeds, the left and right endocardial cushions push in and narrow that space, the dorsal and ventral endocardial cushions are pinching together on the midline and closing the ostium primum. 00:37 But we can also see that the ventricular muscular septum is growing upward, so the muscular portion grows towards the endocardial cushions and would make all the sense in the world if it just kept on growing not the endocardial cushions and separated the two ventricles, but that's not what happens. 00:56 What it does is it leaves a small gap just above the muscular portion and below the endocardial cushions and that is gonna be closed when a portion of the endocardial cushions grows down to meet the muscular portion and that is gonna be called the membranous portion of the interventricular septum and it's gonna form a completely separate left ventricle and right ventricle. 01:23 But fortunately at this time, we've separated the right and left atria, we've separated the right and left atrioventricular canals and now have flow of blood from the inferior vena cava and superior vena cava to the right atrium. 01:37 From there, deoxygenated blood will pass to the right ventricle and then oxygenated blood is coming through the inferior vena cava passing through the foramen ovale to the left atrium then the left ventricle and there will be pushed out to the rest of the body. 01:53 We'll discuss how the aorta and pulmonary trunk separate and also connect to the right and left ventricles in a subsequent talk. 02:02 Now, what can go wrong? Ventricular septal defects are actually one of the most common heart defects and the pseudomembranous version of it is the most common cardiac defect. 02:15 In this case, the endocardial cushions fail to grow down to meet the muscular septum between the two ventricles so we have an open space between the right and left ventricles. 02:29 This causes a shunt of blood from the left to the right after the person is born. 02:35 We can also have defects in the muscular wall although they're less common, but result in a similar shunting of blood and the very rare supracristal ventricular septal defects occur very close to where the aortic and pulmonary valves are located. 02:51 So small ventricular septal defects are sometimes asymptomatic and can in fact close spontaneously, so they may not necessarily have to be operated on right away but could be tracked over the first few years of life to make certain that they do close, otherwise, they can be surgically corrected. 03:08 Large gaps are gonna cause a massive left-to-right shunt as the pressure in the left ventricle becomes much greater after birth. 03:16 Eventually, that shunting of blood from the left to the right will cause right-sided heart failure because the right side of the heart is not really made to handle that kind of pressure and pumping that volume of blood, and surgical correction will almost certainly be necessary. 03:33 Now, we've talked about closure of the atria, closure of the atrioventricular canal and closure of the right and left ventricles from one another. 03:43 One way this can be assessed is by ultrasound and you can get a good look at this process by doing a fetal cardiac ultrasound and you can see that if everything's going to plan, you have that cross-shaped or lower case T-shaped connection. 03:59 So we have a complete atrioventricular separation because the two limbs of the T are meeting continuously. 04:06 The two ventricles are visually, completely distinct from each other because there's a septum there and the left and right atria are separate as well. 04:15 So we can see that in this case everything's worked up pretty well and that simple ultrasound demonstration can show that no atrioventricular septal defects exist or no other any atrioventricular canal defects. 04:28 So prenatal ultrasound is a very important screening device not only to chart and keep track of possible cardiac anomalies, but possibly you have to be ready to repair them the moment the child is born, if necessary. 04:42 Now the valves in the atrioventricular area both on the right side, the triscupid valve, and the left side, the bicuspid or mitral valve, are formed from the endocardial cushions and endocardial cushion defects are often associated with problems of the atrioventricular valves. 04:59 The chordae tendineae and papillary muscles that anchor those valve leaflets to the ventricular wall do not grow upward from the ventricle, but rather are sculpted or almost eroded out of the ventricular wall. 05:14 As the heart enlarges, those muscles remain in place and space hollows out around them. 05:20 So amongst things that can go wrong in this process would be tricuspid atresia. 05:25 Now, this diagram is showing us how blood flow through the normal mature heart is taking place. 05:32 The oxygenated blood comes in through the right atrium from both the inferior and superior vena cava, passes the tricuspid valve to the right ventricle that's pumped to the pulmonary trunk to the right and left pulmonary arteries, they go to the lungs. 05:48 Blood is oxygenated there and comes back through the left and right pulmonary veins to the left atrium. 05:55 This oxygenated blood is then pumped into the left ventricle through the bicuspid valve and then out through the aorta to perfuse all the tissues of the body with well-oxygenated blood. 06:06 Failure of the atrioventricular valve to develop on the right side, tricuspid atresia is absolutely incompatible with further life if there are no other cardiac defects because that would mean there's no way for deoxygenated blood to leave the right atrium and go anywhere. 06:25 However, if there's an atrial septal defect, and ventricular septal defect both at the same time, or an atrial septal defect and a patent ductus arteriosus, that blood can push its way through the atrial septal defect to enter the left atrium. 06:45 At that point, we've got mixing of oxygenated and deoxygenated blood there for cyanosis, bluish tinge of the person's skin, gums, etc. 06:54 And that blood is going to be pushed from the left atrium into the left ventricle. 06:59 And typically, the left ventricle will have to be enlarged because the right ventricle is going to be very, very atrophied by the fact that there's no tricuspid valve there. 07:08 From there, the left ventricle will pump and push blood to both the aorta, and the pulmonary trunk. 07:15 Meaning we've got poorly oxygenated blood going to the body. 07:19 And we have just a little bit of blood making it through the pulmonary trunk to get oxygenation to return to the left atrium. 07:26 So tricuspid atresia will have to be surgically corrected, if it's correctable. 07:31 Thank you very much and we'll return to discuss how the outflow tracks the heart develop, and finish off cardiac development.
About the Lecture
The lecture Separation of Ventricles by Peter Ward, PhD is from the course Development of Thoracic Region and Vasculature.
Included Quiz Questions
The muscular portion of the interventricular septum is derived from which structure?
- Ventricle
- Left endocardial cushion
- Right endocardial cushion
- Dorsal endocardial cushion
- Ventral endocardial cushion
What is the most common congenital heart defect?
- Ventricular septal defect
- Atrial septal defect
- Patent foramen ovale
- Mitral atresia
- Tricuspid atresia
What is the most common type of ventricular septal defect?
- Perimembranous
- Inlet
- Muscular
- Conoventricular
- Supracristal
What heart defect prevents blood flow from the right atrium to the right ventricle?
- Tricuspid atresia
- Mitral atresia
- Ventricular septal defect
- Complete atrioventricular septal defect
- Atrial septal defect
Author of lecture Separation of Ventricles

Peter Ward, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
