Playlist
Show Playlist
Hide Playlist
Reactive Arthritis: Diagnosis and Management

-
Slides Seronegative Arthropathies.pdf
-
Reference List Rheumatology.pdf
-
Download Lecture Overview
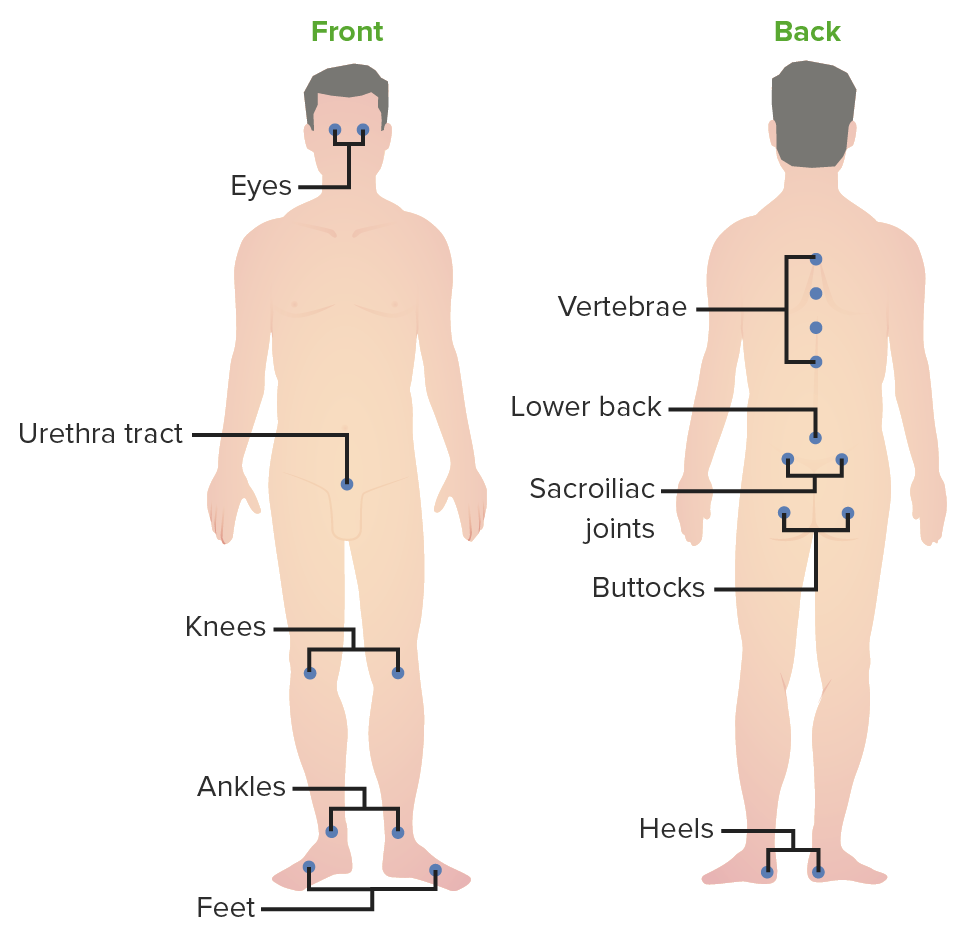
00:00 Alright, so let's review a few key points in our case that will help to highlight some key points about reactive arthritis. 00:08 First of all, we see that she had left knee, left ankle and several toes were involved and that is pretty typical of reactive arthritis. 00:16 You're going to see Oligoarticular arthritis of the lower extremities sometimes called additive arthritis because from one day to the next, a new joint is added to the list. 00:27 Secondly, we talked about the fact that the sole of her left foot is indicative of plantar fasciitis. 00:32 A brief sidebar comment about how to manage plantar fasciitis. 00:36 We typically use night splints which basically lock your heel into a dorsiflex position so that the plantar fascia doesn't constrict overnight. 00:45 Heel stretching exercises can be helpful NSAIDs as needed occasionally we also do direct steroid injections into the plantar fascia insertion at the calcaneal tubercle. 00:57 Next up the fact that her aunt has psoriasis, this is a Family of diseases and so if you have family members who have these diseases you're certainly more likely to be carrying the HLA b 27 haplotype. 01:09 So that is relevant piece of family history. 01:12 Low back pain, as I mentioned, the spondyloarthritides. 01:16 Spondylosis refers to disease of the spine, you're going to see some evidence of low back pain pretty much universally amongst these four conditions. 01:24 In addition, the evidence of Sacroiliitis with pain radiating into the buttocks would be supportive. 01:32 Now, this episode of diarrhea is interesting. 01:36 You may remember that more often than not when we think of reactive arthritis. 01:40 We're thinking about a preceding genital urinary infection in particular chlamydia. However, it's been shown that in addition to those genital urinary sexually transmitted diseases that can precipitate reactive arthritis a lot of the time it's actually a proceeding gastrointestinal illness in particular Shigella, Campylobacter, Salmonella and Yersinia So oftentimes, you'll see that a patient had simply a diarrheal episode a few weeks before the onset of their reactive arthritis picture. 02:09 That being said, as we've mentioned before, inflammatory bowel disease related Spondyloarthritis is also a possibility. 02:17 These symptoms could be the harbinger of the future development of IBD. 02:20 So that's something to keep in mind. 02:22 Just to highlight the commonly involved sites or reactive arthritis we've talked about the knees, the ankles, the toes, and highlighted in the red circles there on the top is where the Achilles tendon would insert into the calcaneus. 02:36 In the bottom circle, is where the plantar fascia inserts into the calcaneus tubercle. 02:42 Other associated findings that you might see with reactive arthritis of course, just like all the Spondyloarthritides, you can see Uveitis and conjunctivitis genital urinary symptoms like urethritis and Cervicitis are common especially if chlamydia was the preceding infection that led to reactive arthritis. 03:01 Remember the old adage, reactive arthritis was can't see, can't pee, can't climb a tree, referring to the Uveitis, the urethritis and the arthritis that goes along with reactive arthritis. 03:12 Next up is the dermatologic manifestations. 03:14 We've talked about aphthous ulcers in the mouth. 03:17 Then the other two, there are these kind of rare birds that we do see associated the reactive arthritis, there's Keratoderma blennorrhagicum which is a desquamating lesion that you'll find on the sole of the feet and then Circinate Balanitis which has these roundish lesions that are appearing on the tip of the penis. 03:37 Okay, now that we've made this diagnosis, how are we going to manage it? You want to check HIV, and that's for two reasons. 03:44 Number one, if you think that person had a sexually transmitted infection with chlamydia it's just good practice to check all of the sexually transmitted infections. 03:52 But more importantly, there's a really high association between being HIV positive and developing reactive arthritis. 03:59 So it's worth just being thorough. Next up like all the Spondyloarthritides, NSAIDs are going to be your first line management glucocorticoids can be used as needed. And then worst case scenario you can add on some of the non-biologic disease modifying anti rheumatic drugs as well. 04:18 Reactive arthritis key points. 04:21 It is preceded by a genital urinary or gastrointestinal illness about one to four weeks prior to all the other symptoms. 04:29 It's an acute, asymmetric, additive, Oligoarticular arthritis look for disease of the eyes, the joints, the tendons, the skin, urethritis and other systemic manifestations. 04:43 It is a seronegative arthropathy that is the rheumatoid factor should be negative you will see some nonspecific inflammatory markers and of course it is associated with the HLA b 27 Allele. 04:55 Lastly NSAIDs and glucocorticoids are your first line treatments for this condition.
About the Lecture
The lecture Reactive Arthritis: Diagnosis and Management by Stephen Holt, MD, MS is from the course Spondyloarthritides.
Included Quiz Questions
Which of the following dermatologic conditions may be associated with reactive arthritis?
- Keratoderma blennorrhagicum
- Keratoacanthoma
- Seborrheic keratosis
- Seborrheic dermatitis
- Actinic keratosis
Which of the following is most commonly associated with reactive arthritis?
- Urethritis
- Balanitis
- Pyelonephritis
- Lichen sclerosus
- Glomerulonephritis
Which of the following is the best initial management for reactive arthritis?
- Ibuprofen
- Azithromycin
- Colchicine
- Allopurinol
- Doxycycline
Author of lecture Reactive Arthritis: Diagnosis and Management

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
