Playlist
Show Playlist
Hide Playlist
Placental Abnormalities


-
Slides PregnancyComplications Female ReproductivePathology.pdf
-
Download Lecture Overview
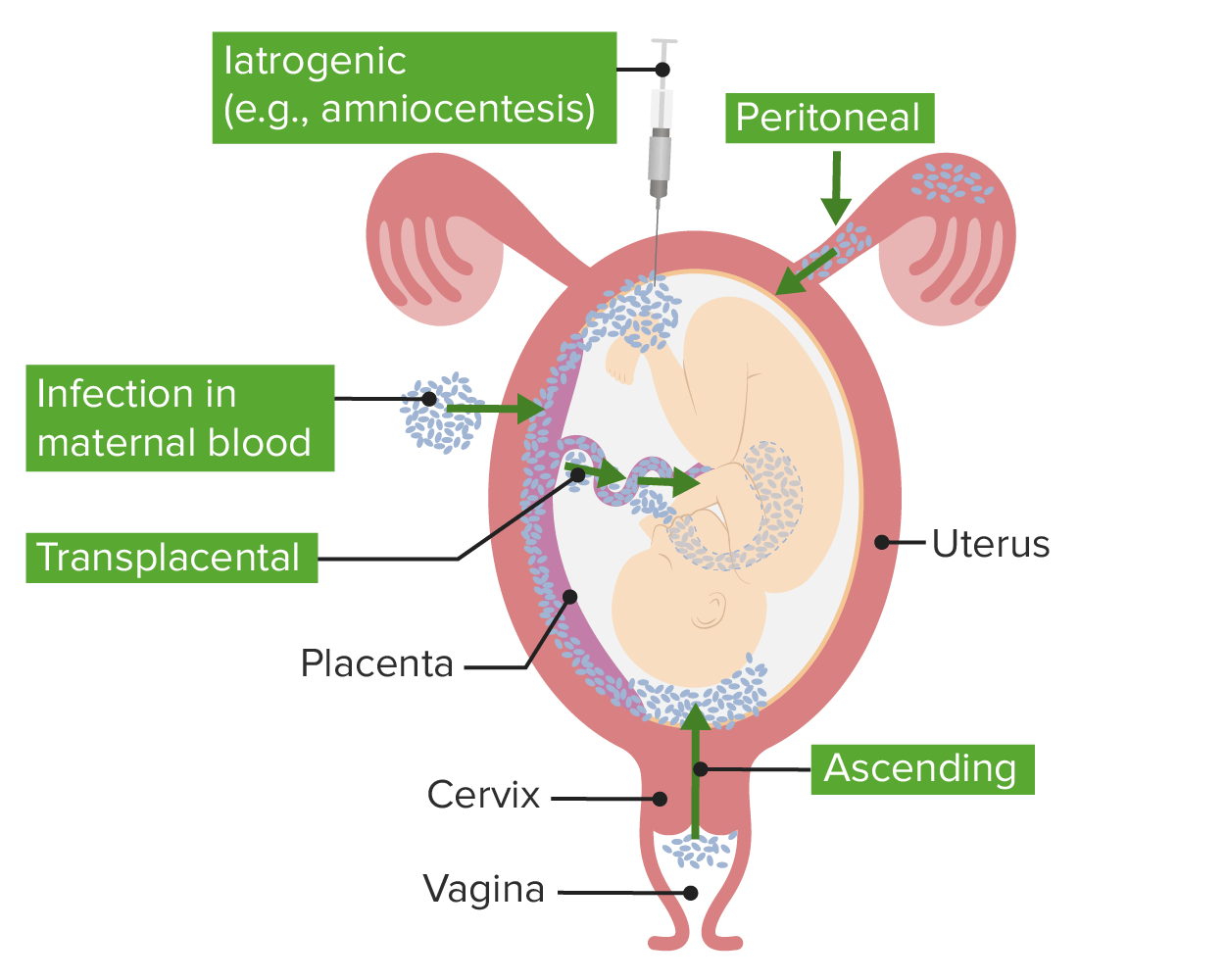
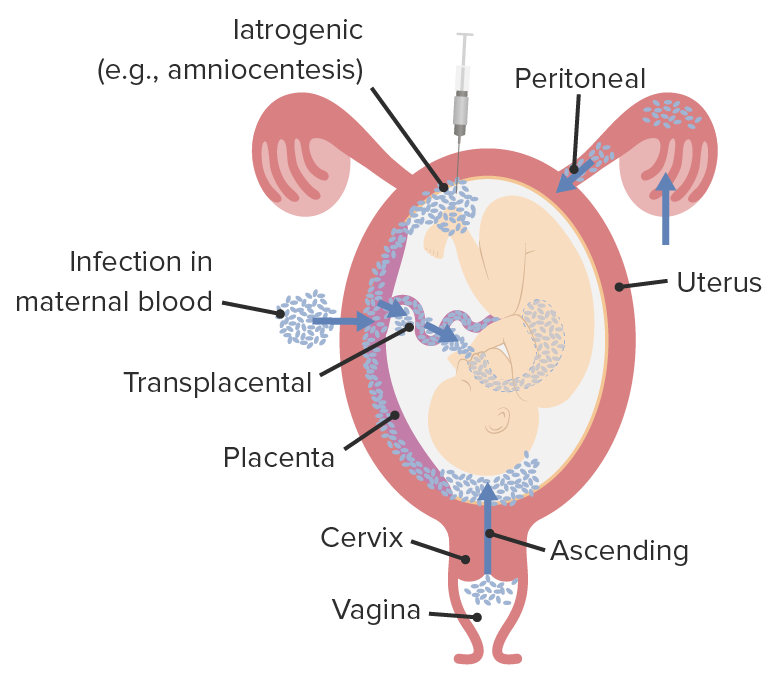
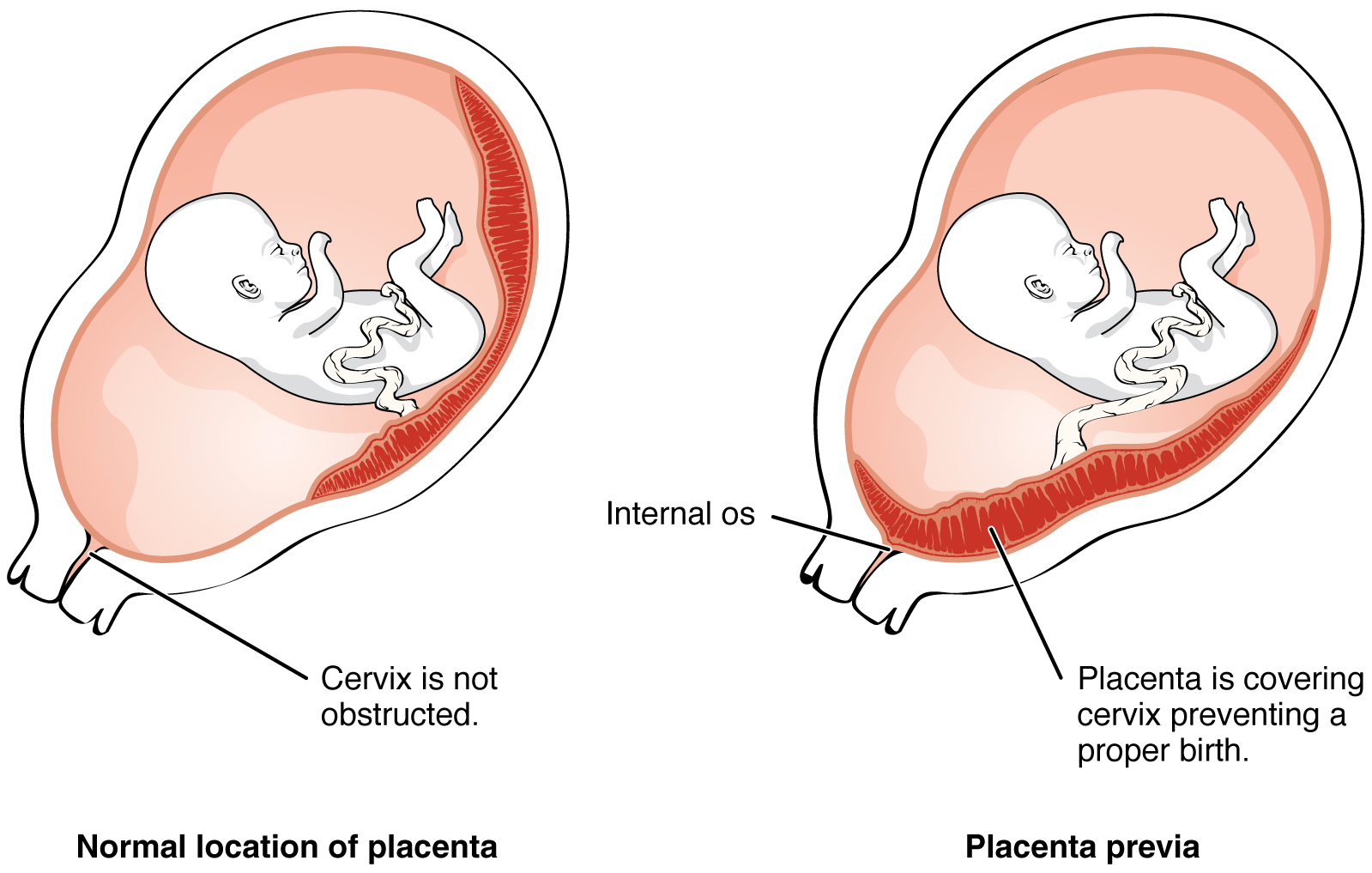
00:01 Our topic now brings us to various placental abnormalities. 00:05 I will walk you through those placental abnormalities that you will encounter on a frequent basis. 00:12 Our first diagnosis here will be placenta accreta. 00:16 Once we understand accreta, then I’ll quickly tell you about others that share the name and we’ll tell you exactly as to where the placenta is then attaching. 00:27 The reason I emphasized "attaching" is because accreta has the letter A in it. 00:32 It is going to attach to what? Now that’s the pathology that I will describe to you. 00:39 What ends up happening is that normally, if you have implantation in the uterus. 00:43 Now, this is not ectopic pregnancy. 00:46 The fertilized egg has made its way to the uterus and this time, normally speaking, this fertlized egg should implant and attach to the decidua. 00:57 The decidua is part of the endometrium of the female uterus. 01:01 Think of it as such. 01:03 What ends up happening here – Well, what’s the next superficial layer of the uterus? It’s called the myometrium, correct? My goodness, there should be no implantation or attachment to the myometrium. 01:15 But if that occurs, this brings you to the diagnosis of placental accreta. 01:20 Partial or complete absence of decidua, which means that the normal endometrium tissue that should be attaching to the chorionic villi of the placenta is not occurring. 01:33 Therefore, you’ll notice here that the placenta is directly attaching to the myometrium. 01:39 Once you understand that, let’s go on to complications here and you’ll find this be quite interesting and makes perfect sense. 01:46 If you have a placenta that’s attaching the myometrium, that is a very firm and pathologically strong attachment to the myometrium. 01:57 So now it’s time for delivery, parturition. 02:01 And so therefore the placenta is having a hard time coming off the myometrium. 02:06 What does that mean? That means that now, perhaps if it finally detaches, you have complications because now you might cause tearing and there might be massive hemorrhage. 02:18 So now you tell me, as soon as you hear about placental abnormalities and in complications, and you’re thinking about hemorrhage, What’s going on with your patients? Both the fetus, the newborn, and perhaps the mother? The mother is experiencing Sheehan syndrome. Clear? So that will be the scenario or that will be the type of scenario that you’re going to get with pituitary infarction in the mother. 02:43 This will be a good one for you to put all of that together. 02:47 Predisposed by inflammation or scarring. 02:50 Causes postpartum bleeding. 02:52 Keep in mind that this may then result in pituitary infarction of the mother. 02:57 We call this Sheehan. 02:59 Associated with placenta previa as well, which will be a separate topic upcoming. 03:05 But we know accreta. 03:07 And I told you earlier that once you understand the foundation of accreta and where it attaches to, then we’ll talk about other attachments. 03:15 And meaning to say that instead of attaching to the myometrium, it might then infiltrate or invade, you call that increta. 03:22 Or perhaps, you even – Not only do you invade, but then you perforate. 03:26 That’s called perforeta. 03:29 Understand the foundation though. 03:30 Accreta, not -- not -- attaching to the normal decidua and so therefore from here, you can go into accreta, increta and perforeta. 03:44 A placental abnormality known as placenta previa. 03:48 I’d like for you to take the "V" in previa and take a look at the shape and work with me here, I’ll make your life easier. 03:56 I want you think of that V as being the uterus. 03:59 And the bottom of the V, it converged to a single point. 04:03 I want you to go ahead and imagine the uterus and you’re going t converge into the cervix, aren’t you? So the V, think of it as being the cervix, the convergence point. 04:15 Normally speaking, the placenta should be attaching to the proximal portion of the fundus. 04:20 The wide body portion of the fundus, correct? Instead of that, you have the placenta, which is attaching down by the cervical os. 04:30 Now can you imagine as to what that pathology looks like? Placenta implants in lower uterine segment or cervix with serious antepartum bleeding here as well. 04:41 So many of your placental abnormalities that we had been looking at including accreta and we have previa, may be associated with bleeding taking place. 04:50 Understand the foundation of previa and that from here, you could either have partial or complete type of previa, But at this point, I’m just going to walk you through the fundamentals. 05:04 Here, you have a patient who -- A pregnant woman, who gets infected with whatever organism. 05:12 Now, what ends up happening is the fact that the chorio -- We’re going to split this up for you. 05:17 The chorio means the side of the fetus and specifically referring to the placenta. 05:24 And the finger-like projections of the fetal placenta is known as your chorionic villi. 05:31 Chorionic villi. 05:33 Think of that as being like fingers. 05:36 I’m just speaking generally. 05:38 Fingers. Villi. 05:39 And the chorionic villi of the placenta is responsible for extracting the oxygen from the mother, okay? What may then happen is the fact that the chorioamnion, once it becomes infected, you call this chorioamnionitis. 05:55 This is not good. 05:57 It follows premature rupture of the membrane. 06:00 Usually due to an ascending infection. 06:03 What ascending infection? Are you picturing this? There’s an infection taking place from the vagina, maybe a sexually transmitted infection making its way up the vagina, up the cervix, and oh my goodness, it’s affecting the fetus, specifically the placenta. 06:18 Even more specific, chorionic villi. 06:20 Now we have chorioamnionitis. 06:23 If you have rupture of such membranes, what’s going to happen? Early birth, pre-term. 06:29 And upon such preterm babies being delivered, obviously these are low birth or perhaps even very low birth weight and that’s a problem, isn’t it? It could be a host of complications including neonatal respiratory distress syndrome, so on and so forth. 06:45 You see as to how everything’s being connected here. 06:47 We can’t just memorize one thing at a time. 06:49 It’s all about, well, what are the consequences that may occur following.
About the Lecture
The lecture Placental Abnormalities by Carlo Raj, MD is from the course Pregnancy Complications.
Included Quiz Questions
Which term describes a placenta that is directly attached to the myometrium?
- Placenta accreta
- Chorioamnionitis
- Low anterior placenta
- Abruptio placentae
- Placenta previa
Which of the following is NOT associated with placenta accreta?
- Rupture of fallopian tubes
- Sheehan syndrome
- Inflammation and scarring of the uterine lining
- Absence of the uterine decidua
- Postpartum hemorrhage
What is placenta previa?
- A placenta that implants in the lower uterine segment or cervix
- A placenta that implants into the myometrium
- The first villi that attach to the uterus
- A placenta that attaches to the decidua too early
- A placenta that goes through the serosa to surrounding organs
What is a major risk factor for chorioamnionitis?
- Preterm prelabor rupture of membranes
- Placenta previa
- Placenta percreta
- First pregnancy
- Urinary tract infection
Author of lecture Placental Abnormalities

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
