Playlist
Show Playlist
Hide Playlist
Peripheral Neuropathy: Parts of Nerves Involved


-
Slides Introduction to Neuropathy Disorders.pdf
-
Download Lecture Overview
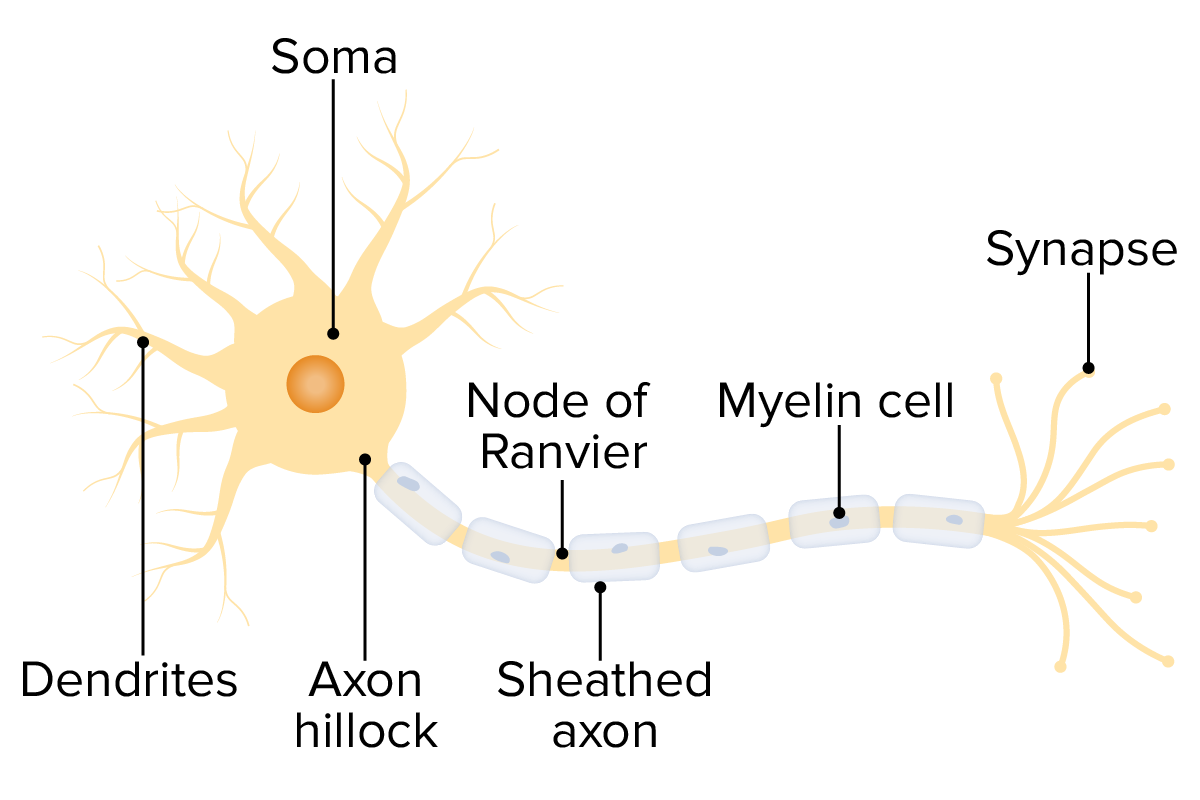
00:01 When we categorize peripheral neuropathies, we want to walk through that in three steps. 00:06 The first step is to understand the part of the nerve that is involved, the second is to evaluate the type of the nerves that's involved, and our third approach can be to evaluate the size of the nerve that's involved. 00:18 We want to look and think about the part, the type, and the size of nerve involvement. 00:22 So, let's walk through each of those. 00:24 When we're thinking about the part of the nerve, we're thinking about proximal and distal nerve involvement. 00:29 The most proximal part of the nerve is the nerve root, and disorders that affect the nerve root include radiculopathies where a single nerve root is involved, or a polyradiculopathy where multiple nerve roots are involved. 00:42 The most common example of a radiculopathy is a herniated disc, where the disc pushes on a single nerve root, and this results in dysfunction along the myotome and dermatome of that nerve root. 00:53 The most common polyradiculopathy is Guillain-Barre syndrome, which was present in the patient in our case, and that's where multiple nerve roots are affected by an inflammatory process in the nerves. 01:05 And so, the classic polyradiculopathy is Guillain-Barre syndrome or acute inflammatory demyelinating polyneuropathy. 01:12 If we can figure out whether the nerve root is involved, we can narrow our differential diagnosis. 01:18 The next part of the nerve is the nerve plexus. 01:21 Problems in the nerve plexus affect both the motor and sensory nerves, and so patients are weak and report problems with sensation, and some common examples of things that affect the nerve plexus include radiation plexitis in cancer patients, diabetic amyotrophy, which occurs in patients with diabetes, and Parsonage-Turner syndrome, which is an inflammatory disorder of the nerve plexus. 01:45 If we can localize the problem to the plexus, then we can narrow our differential diagnosis to things that commonly affect and have tropism for that area. 01:54 And then, the last part of the nerve is the terminal nerve branches, and things that affect the terminal nerve branches include diabetes, alcohol-induced polyneuropathy, and inherited polyneuropathies like this Charcot-Marie Tooth syndromes. 02:06 We can also localize problems to the type of nerve that's involved. 02:12 There are sensory neuropathies, motor neuropathies, and autonomic neuropathies, and by using our history and exam to narrow the problem to sensory, motor, or autonomic nerves, we can narrow our differential diagnosis. 02:25 Some common sensory only neuropathies or sensory ganglionopathies are the paraneoplastic neuropathies. 02:32 Anti-Hu antibody syndrome is a good example of a sensory only problem. 02:36 Patients present with problems with vibration and proprioception and rarely pain and temperature function, but they're perfectly strong. 02:43 Their reflexes are reduced or areflexic as a result of that sensory arc of the reflex exam, but it's a sensory only process. 02:52 There are a number of motor only neuropathies which are called motor neuronopathies and a classic example is a Guillain-Barre variant, acute motor axonal neuropathy where just the motor nerves are involved. 03:04 Patients present with weakness, often with hypo or areflexia without any sensory involvement. 03:10 And if we can prove that the sensory nerves aren't involved, we can narrow our differential to motor only neuropathies. 03:16 And then, autonomic neuropathy is commonly seen in a variety of sensory neuropathies, motor neuropathies, or autonomic only neuropathies. 03:23 Diabetes is a good example where we often see early autonomic dysfunction, constipation, erectile dysfunction, orthostasis, and other evidence of autonomic nerve dysfunction. 03:34 We can also localize neuropathies to the part of the nerve that's involved. 03:38 Is it the axon or is it the myelin? There are a number of axonal polyneuropathies. 03:44 An example of that is acute motor axonal neuropathy where just the axon is affected, but the list of axonal neuropathies is extremely long. 03:52 We use EMG nerve conduction study to differentiate axonal and demyelinating neuropathies, and if we can prove that this is an axonal only process, we can pull out that list and evaluate those causes of an axonal neuropathy. 04:06 There are also a number of conditions that primarily affect the myelin and result in demyelinating neuropathies. 04:13 The classic example is acute inflammatory demyelinating polyneuropathy. 04:17 Demyelinating neuropathies are often immune mediated, and they come from an autoimmune disorder from an infection that sets off the immune system or a paraneoplastic process. 04:27 When we see evidence of demyelination on the nerve conduction study, we can think about that differential diagnosis of demyelinating neuropathies and often treat the immune system or activation of the immune system to improve symptoms in those patients. 04:43 And we can also think about the size of nerve involvement and characterizing neuropathies as large or small fiber can narrow down the differential and drive our diagnostic investigation and treatment. 04:53 A classic large fiber neuropathy is anti-Hu antibody, paraneoplastic polyneuropathy, and again, those large fibers carry information about vibration and proprioception. 05:04 Problems with vibration and proprioception with sparing of pain and temperature points us to one of these large fiber neuropathies. 05:13 Small fiber neuropathies present with prominent pain and temperature dysfunction. 05:18 Patients often have significant neuropathic pain, burning, paresthesias, numbness, or electric shock like sensations, and a classic example of a small fiber neuropathy is chemotherapy induced peripheral neuropathy.
About the Lecture
The lecture Peripheral Neuropathy: Parts of Nerves Involved by Roy Strowd, MD is from the course Introduction to Neuropathy Disorders.
Included Quiz Questions
Which of the following is likely to be caused by a herniated disk?
- Single nerve root radiculopathy
- A polyradiculopathy
- Autonomic neuropathy
- Radiation plexitis
- Anti-Hu antibody paraneoplastic polyneuropathy
A diabetic patient that exhibits erectile dysfunction, constipation, and orthostasis likely has which of the following?
- Autonomic neuropathy
- Guillain-Barré syndrome
- Parsonage-Turner syndrome
- Acute motor axonal neuropathy
- Alcohol-induced peripheral neuropathy
Which finding or complaint would most likely exclude large fiber neuropathies from the differential diagnosis?
- Bilateral burning foot pain
- A vibratory deficit on exam
- Position sense deficit on exam
- Light touch deficit on exam
- Muscular weakness
Author of lecture Peripheral Neuropathy: Parts of Nerves Involved

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
