Playlist
Show Playlist
Hide Playlist
Pediatric Hirschsprung Disease

-
Slides GD Pediatric GI.pdf
-
Download Lecture Overview
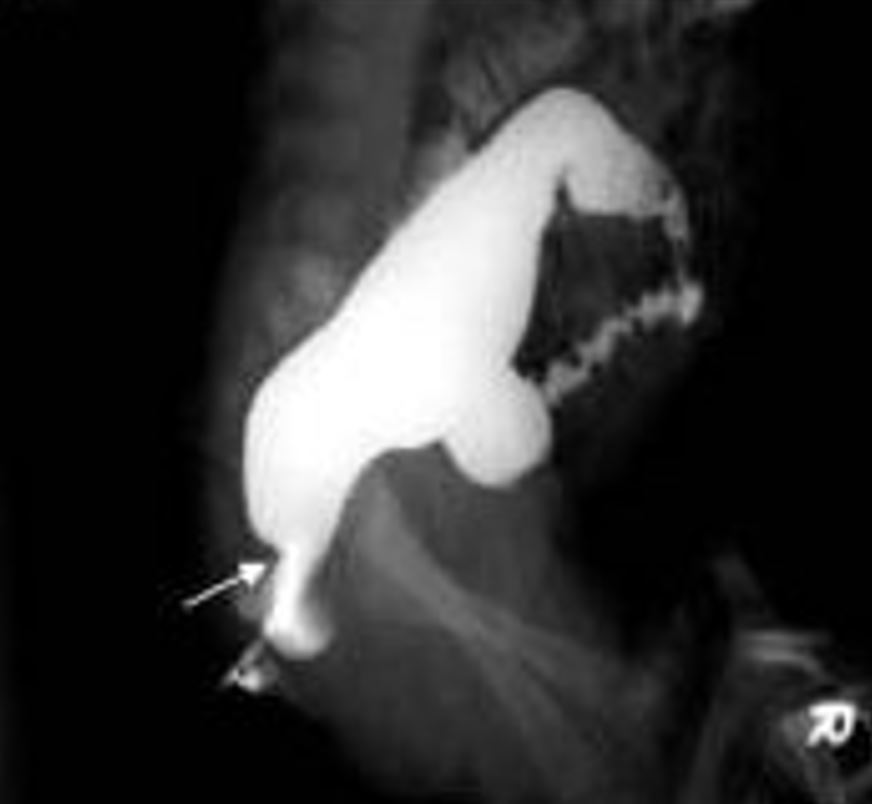
00:01 Our topic is Hirschsprung's disease. 00:04 In other words, this is megacolon. 00:07 Now, Hirschsprung's disease is quite, quite straightforward for the pediatric population. 00:13 There something called the enteric nervous system, do you remember that from physio? That enteric nervous system behaves very much like your parasympathetic nervous system, and by that, we mean you've heard of rest and digest. 00:24 You need the parasympathetic nervous system with having its own pacemaker known as your -- you've heard of the cell -- the interstitial cells of Cajal? And that pacemaker allows for the intestine and really the GI to move forward, propulsion, peristalsis. 00:41 And allows for the sphincters to relax so that you move the food forward, right? Welcome to parasympathetic. 00:48 This muscle contraction that you find, let's say in the esophagus, in the stomach, and in the intestine, all of that is a particular plexus of your enteric nervous system and that plexus that I'm referring to is – What is it? Good. 01:05 The myenteric plexus, a.k.a. Auerbach plexus. 01:10 That's the plexus that you should be focusing upon in Hirschsprung's disease and specifically enteric nervous system because that's the muscle plexus that allows for contraction. 01:22 What gives rise to enteric nervous system embryologically? It's called the neural crest cells? If the neural crest cells do not migrate properly down in the intestine, You are not going to develop your myenteric plexus properly. 01:36 Uh-oh. 01:37 So if myenteric plexuses are not present in that part of the intestine, you’re not going to have contraction. 01:44 You tell me. Is this a functional type of constipation or is this going to be an obstructive type of disease. 01:53 This is actual functional obstruction, not mechanical. 01:56 You've lost your plexus. 01:58 Failure of neural crest cells. 02:00 Therefore, this is a functional obstruction because you can't move forward. 02:04 Welcome to megacolon. 02:07 Constipation in a neonate should be considered Hirschsprung's disease until proven otherwise. 02:12 That is how important this is. 02:14 Constipation in a neonate. 02:16 Look at your population here. 02:17 Neonate. 02:18 Remember the three populations, you have your neonate and had your infant and then you had your child going into adolescence. 02:27 What do you want to do to confirm your diagnosis of Hirschsprung? You do a biopsy. 02:32 So now, use common sense, here's your intestine and the enteric nervous system isn’t there. 02:39 The myenteric plexus is absent. 02:42 Therefore, upon biopsy of that region, that has now become damaged or is not moving, you'd expect to find no ganglion cells. 02:53 Absence of ganglionic cells or aganglionic segment. 02:58 So what then happens, here's my functional obstruction. 03:02 If things don’t move forward, what are you going to find proximally? Anytime you have obstruction distally, proximal dilation. 03:11 Hence, we call this megacolon. Hirschsprung. 03:15 Hirschsprung. 03:16 Now, it's one cause of megacolon. There are other causes and, for example, you could have an adult who then suffers from Chagas' disease and that will be obviously Trypanosoma cruzi. 03:27 But here specifically with pediatric neonate, and you're thinking about Hirschsprung, failure of neural crest cells. 03:34 You'll notice the following here on x-rays. 03:36 The first on your left pretty much showing a massive megacolon. 03:41 Massive Megacolon. 03:43 And on the right, you'll notice there as well, that is a massive megacolon. 03:47 And distally, you'll find that things are a little bit more narrowed. 03:52 If you were to then take the area that's narrowed, that's the area of the pathology, not the dilated part. 03:59 The dilated part wants to contract, but it can't move forward because the distal portion doesn’t have the myenteric plexus. 04:07 So that area that is narrowed distally, You do a biopsy of that and you're not going to find what? Ganglion cells. 04:16 Good. 04:19 Hirschsprung. Management: Surgical resection of affected segment of bowel, really it's the only option that you have at this point. 04:27 Definition, absence of ganglionic cells, so therefore you've lost –- or the intestine -- has lost the autonomic innervation and thus, resulting in functional obstruction. 04:37 Signs and symptoms is because this is failure of neural crest cells, You are looking at congenital issues, so therefore there's no passage of that early stool. 04:46 In other words, within the first 24 hours, the meconium is not passed. 04:51 Obstruction leads to bowel dilation as I've shown you both on x-ray and on physical specimen as well. 05:01 Your barium enema would show you exactly as to what you'd expect with an enlarged proximal dilation And biopsy once again will show you absent ganglionic cell. 05:12 Management: Surgery.
About the Lecture
The lecture Pediatric Hirschsprung Disease by Carlo Raj, MD is from the course Pediatric GI Pathology.
Included Quiz Questions
Which of the following statements regarding the embryologic association of Hirschsprung disease is TRUE?
- Failure of migration of the neural crest cells into the intestine occurs.
- Failure of migration of the neuroendocrine cells into the intestine occurs.
- Failure of fusion of the neural tube occurs.
- Abnormal accumulation of the neuroepithelial cells occurs.
- Abnormal proliferation of neural blast cells occurs.
Which of the following cells is decreased in Hirschsprung disease?
- Interstitial cells of Cajal
- I cells
- Enteroendocrine cells
- Enterochromaffin cells
- Paneth cells
Which of the following cells is absent in the dysfunctional segment of Hirschsprung disease that can be confirmed by immunohistochemistry?
- Ganglion cells
- The longitudinal layer of the smooth muscles in the distal segment of the intestine
- The horizontal layer of the smooth muscles in the distal segment of the intestine
- The lymphoid aggregates in the distal segment of the intestine
- The lymphoid aggregates in the proximal segment of the intestine
Which of the following parts is considered the pathologic segment in Hirschsprung disease?
- The distal portion of the intestine is the aganglionic segment.
- The proximal portion of the intestine is the aganglionic segment.
- The proximal portion of the intestine is a narrow and affected segment.
- The distal portion of the intestine is the ganglionic segment.
- Both the proximal and distal portion have ganglion cells.
Author of lecture Pediatric Hirschsprung Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
1 customer review without text
1 user review without text
