Playlist
Show Playlist
Hide Playlist
Pediatric Polycystic Kidney Disease



-
Slides PKD Pediatrics.pdf
-
Download Lecture Overview
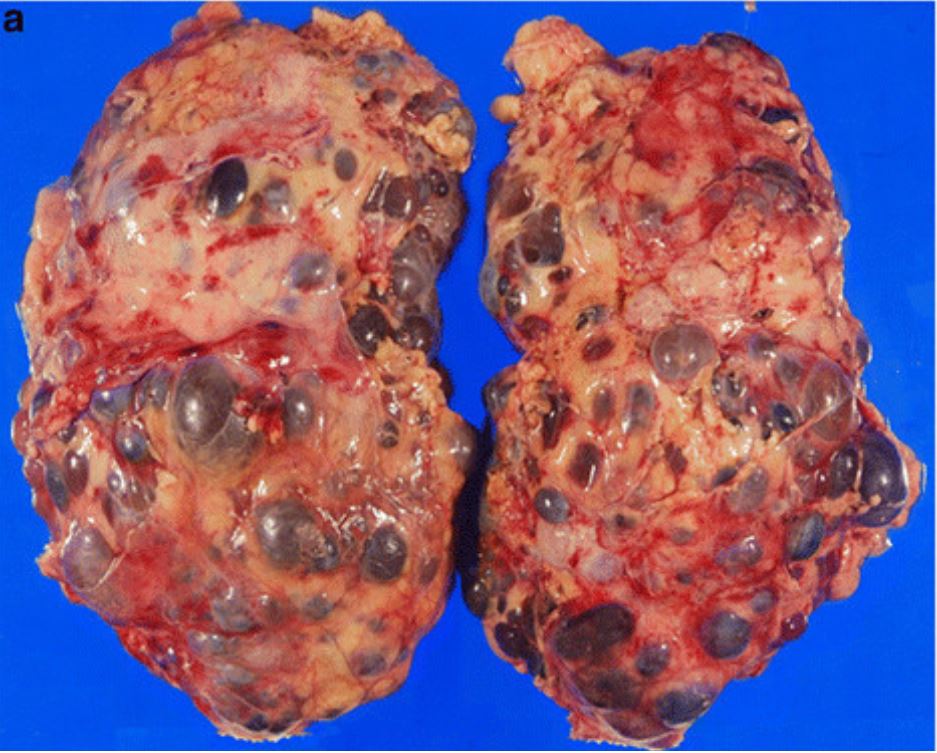
00:01 In this lecture, we’re going to review polycystic kidney disease. 00:05 Polycystic kidney disease comes in two major types: Autosomal recessive and autosomal dominant. 00:13 So autosomal recessive polycystic kidney disease is what we see most often in children. 00:19 It can present congenitally and early in infancy. 00:24 Generally, there is dilatation in this case of the collecting ducts of the kidney resulting in cysts forming in those kidneys. 00:32 These patients may also develop a hepatic fibrosis. 00:36 This is compared to autosomal dominant kidney disease which usually presents in adulthood and worsens with age. 00:45 It’s often diagnosed in adulthood. 00:47 It will be very rare to make this diagnosis in a child unless there was already a family history of the disease. 00:53 Cysts can form in autosomal dominant disease in multiple organs. 00:59 The kidney is certainly involved, but these patients may develop cysts in the liver, the pancreas, et cetera. 01:06 So in autosomal recessive polycystic kidney disease, this is often picked up on prenatal ultrasound. 01:14 This is because the cyst exist in utero as well and they may have a decreased urine output. 01:20 Recall that the amniotic fluid is mostly generated by urine output in utero. 01:26 As a result, because they may don’t have much urine output, these children may present with oligohydramnios in the prenatal period during the routine ultrasound of the child. 01:38 This patient may have abdominal distention, but also they may have hypertension, oliguria, and they may be in respiratory distress from pulmonary hypoplasia as a result of having poor urine output and having less fluid in their amniotic sac. 01:56 This is compared adult onset autosomal dominant polycystic kidney disease which is only incidentally found in childhood and it’s very rare to have symptoms before adulthood, usually around 30 years of age. 02:11 So because the autosomal recessive variety of polycystic kidney disease is the one we see in children and I’m delivering pediatric lectures, I want to focus on the recessive form of infantile polycystic kidney disease. 02:26 Like I said, this is usually noted on prenatal ultrasound and often presents in the newborn period. 02:33 Also, these patients may well have pulmonary hypoplasia. 02:38 Remember that the in-utero environment is important for lung development and in particular, that pressure that is created by amniotic fluid and that is then filtering down into the lungs is necessary for lung development. 02:53 These patients therefore may have pulmonary hypoplasia as well. 02:57 On ultrasound, we will usually find cysts. 03:01 This can be almost diagnostic. 03:03 Patients may often have hyponatremia or increased creatinine from their renal failure. 03:09 Additionally, these patients are increased risk for urinary tract infection and in particular pyelonephritis. 03:16 Genetic testing is available and may be useful in families where this condition has been seen before and they’re worried about having another child with the condition. 03:26 So how do we manage polycystic kidney disease in infants? Well, respiratory support is key, especially for those patients with pulmonary hypoplasia. 03:36 We may put them on dialysis because their kidneys aren’t functioning particularly well. 03:41 These children will often need antihypertensive therapy, again, because of the renal failure. 03:47 Eventually, this may lead to renal transplant. 03:51 Typically, they may just leave the old kidneys in there rather than remove them and simply place a new one. 03:57 In infants, renal transplant may take place in the abdominal compartment as opposed to retroperitoneally. 04:04 The prognosis of these children depends on the severity of their disease and how rapidly they’ve progressed. 04:11 Genetic counseling is important to families so they can understand risks to future children and that may mitigate in some way how future pregnancies are handled. 04:21 So that’s my summary of polycystic kidney disease in children. 04:25 Thanks for your time.
About the Lecture
The lecture Pediatric Polycystic Kidney Disease by Brian Alverson, MD is from the course Pediatric Nephrology and Urology.
Included Quiz Questions
Which of the following statements is TRUE about pediatric polycystic kidney disease?
- It is an autosomal recessive disorder.
- It is rarely noted on prenatal ultrasound.
- It usually presents after the age of 10.
- Pulmonary hypoplasia is a very rare complication.
- Diagnosis is typically made by CT scan.
Which of the following is NOT true regarding congenital autosomal recessive polycystic kidney disease?
- The kidneys are the only site of involvement.
- It is commonly diagnosed prenatally.
- Oligohydramnios is a common finding.
- It is associated with pulmonary hypoplasia.
- Patients have an increased risk of urinary tract infections.
Author of lecture Pediatric Polycystic Kidney Disease

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture. Very well presented. Easy to understand and remember. Thank you!
nice summary of the condition of pediatric polycystic kidney disease
