Playlist
Show Playlist
Hide Playlist
Pediatric Fractures

-
Slides Pediatric Fractures.pdf
-
Download Lecture Overview
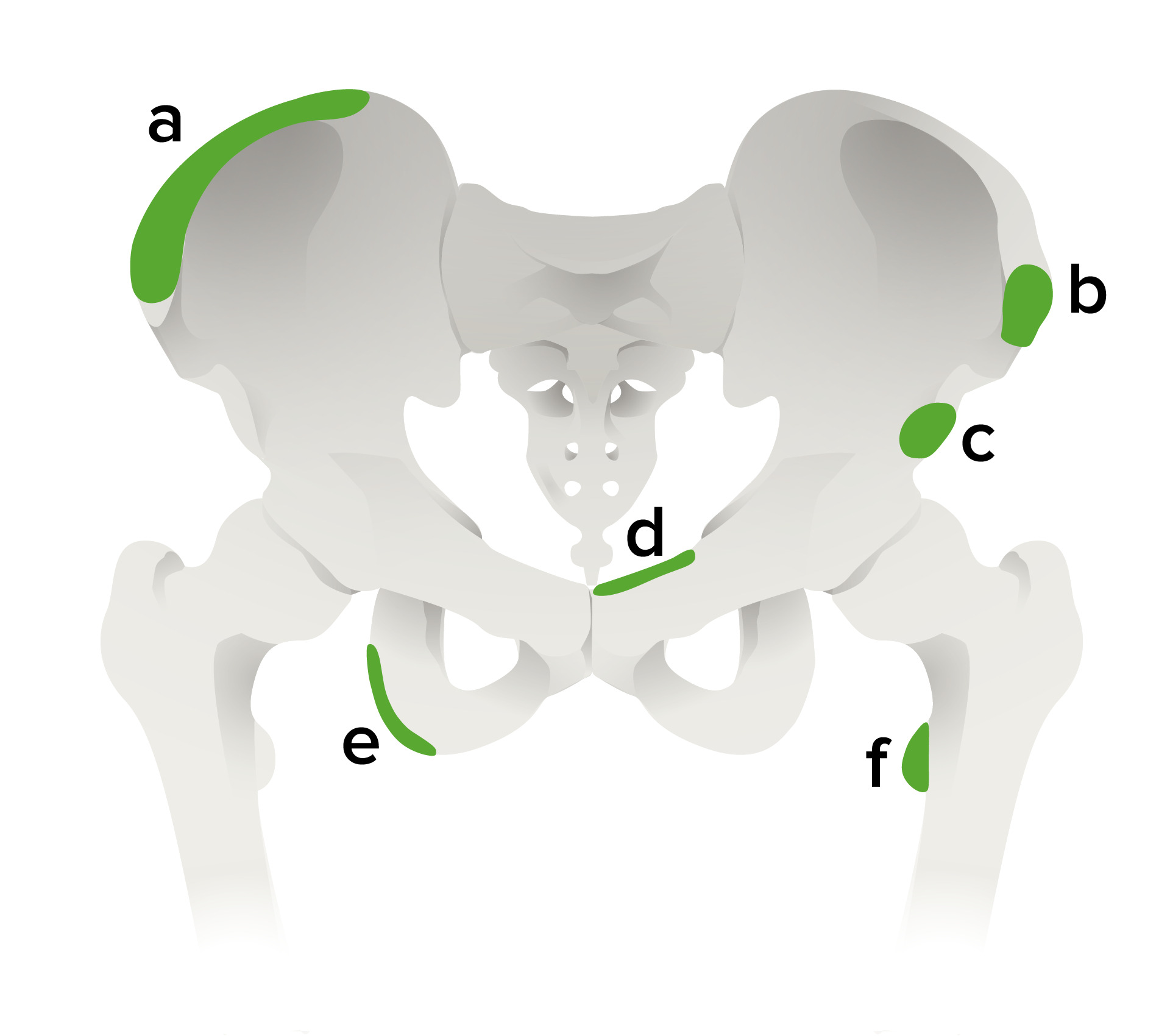
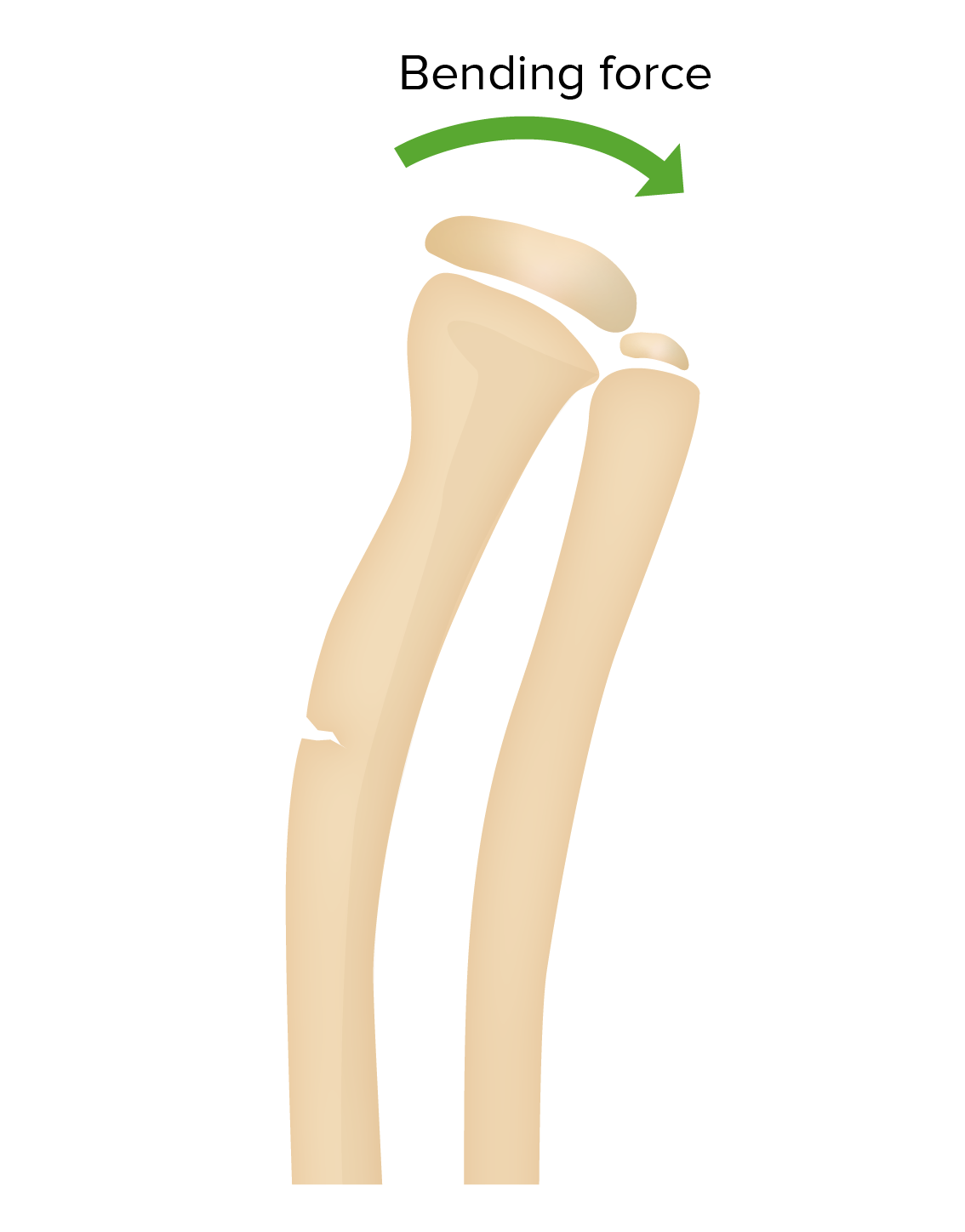
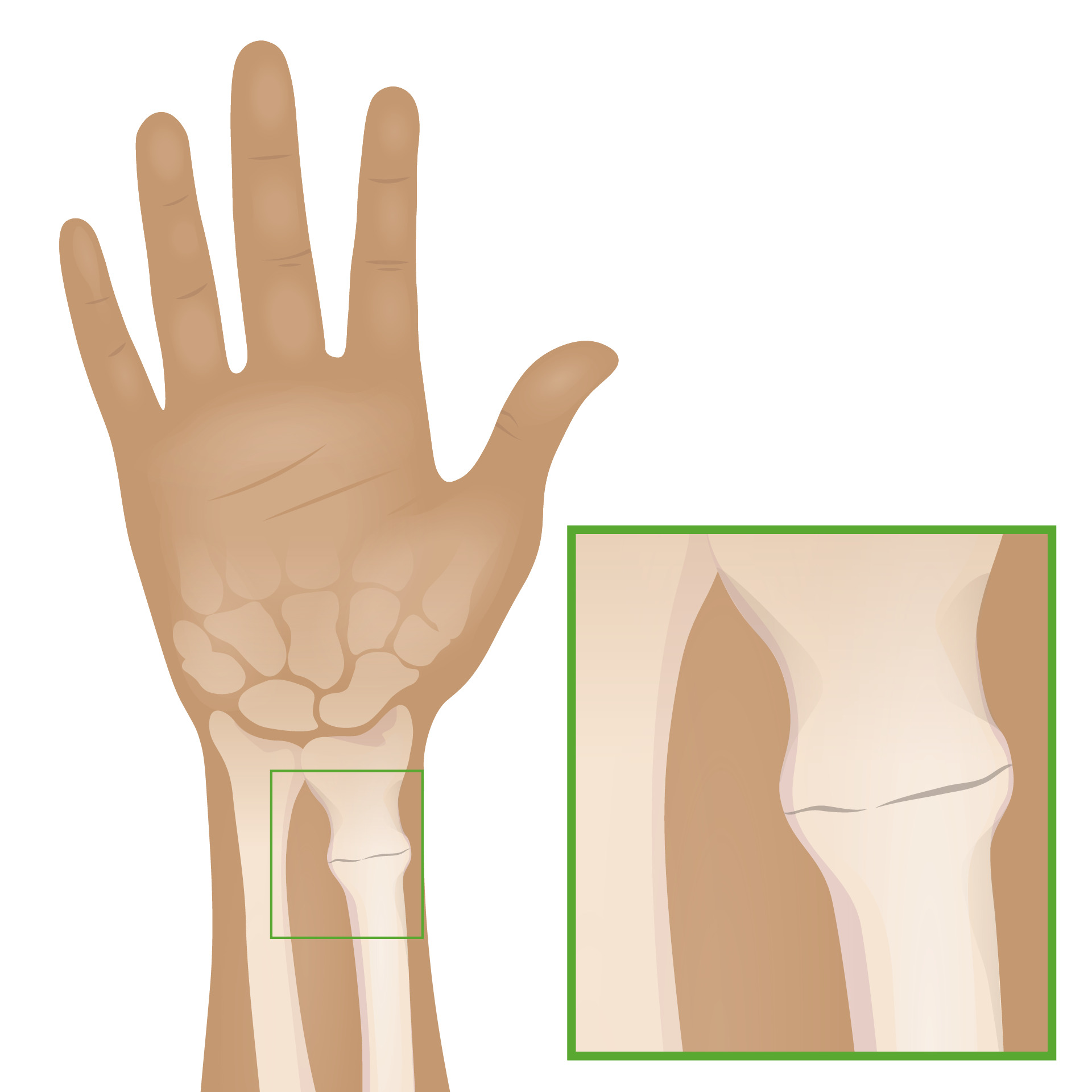
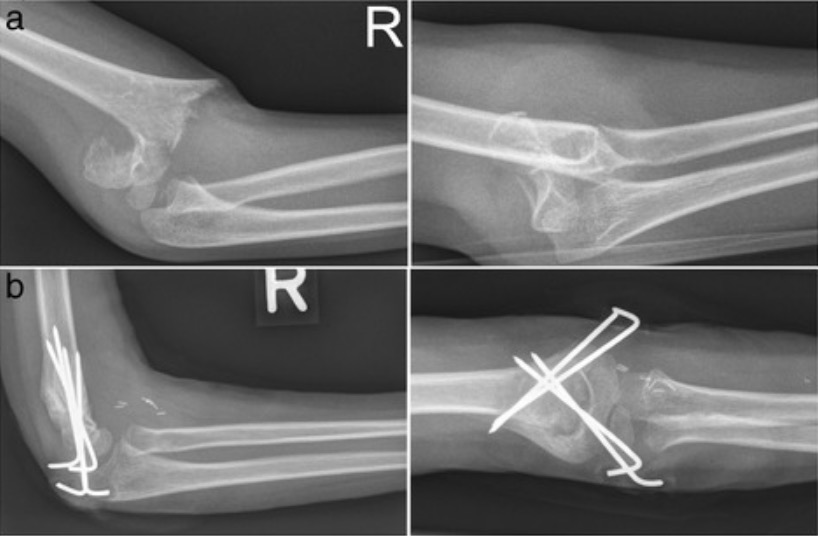
00:01 Pediatric fractures deserve a discussion separate from adult fractures. 00:05 Pediatric bones are skeletally immature and they differ from mature bones because of the presence of an epiphyseal or growth plate. 00:13 The involvement of the growth plate can change the treatment and it can also change the type of complications that can occur from a fracture. 00:19 So the most commonly used classification for pediatric fractures is called the Salter Harris Classification. 00:25 Let's take a look at each of these in a little more detail. 00:28 So Salter Harris Fracture is one that involves the growth plate. 00:32 A Salter Harris II Fracture goes through the growth plate and it goes through the metaphysis. 00:37 A Salter Harris III will go through a portion of the growth plate and the epiphysis and a Salter Harris IV will go through the growth plate, the epiphysis and the metaphysis. 00:48 A Salter Harris V Fracture can go through right through the growth plate but it's more of a crush injury through the growth plate. 00:54 So each of these fractures can have different complications. 00:57 A Salter Harris I may actually be occult on imaging but it has a very good prognosis. 01:02 The Salter Harris Type II is most commonly occurring Salter Harris fracture that also has a good prognosis. 01:09 A Salter Harris III can enter into the joint space and it can result in premature growth plate fusion and osteoarthritis, so this one is important to recognize as the prognosis is not as good. 01:21 With the Salter Harris IV, this also enters the joint space and can result premature growth plate fusion and osteoarthritis, so similar to a Type III which doesn't have a very good prognosis. 01:32 The Salter Harris V Fractures actually have a very poor prognosis because they result in vascular injury and they can cause premature fusion of the growth plate. 01:41 In addition, this can actually be occult on imaging. 01:44 So let's take a look at this radiograph. 01:47 This is an x-ray of the first digit. 01:49 So do you see the fracture and what kind of classification would this be? So the arrow points you to the fracture. 02:01 You can tell that this is a skeletally immature patient because you can see the growth plate open in these bony structures. 02:08 Here you can see the growth plate right here and then this is the fracture right here. 02:14 So this is a fracture of the growth plate that extends through the metaphysis. 02:20 This is a Salter Harris Type II fracture which tends to have a pretty good prognosis and this is also the most common of the Salter Harris fractures. 02:28 So let's take a look at this. This is another example of an x-ray of the first digit. 02:32 This is also a skeletally immature patient. 02:35 So you can see the open growth plate right here and you can see the arrow pointing to the fracture which involves the epiphysis. 02:42 So this is an example of a fracture involving both the growth plate and the epiphysis which is a Type III Salter Harris fracture. 02:49 This does extend to the joint space as you can see because it involves the epiphysis which then extends to the joint space right here, so this can actually cause premature growth plate fusion and osteoarthritis. 03:01 This is a type of fracture that would need close intervention. 03:04 Let's take a look at this. This is an x-ray of the pelvis. 03:07 This is also a skeletally immature patient as you can see the growth plates are open right here on the hips. 03:13 You can see the other growth plate right here. 03:16 So what's the abnormality here? So this is an example of what's called, "Slipped Capital Femoral Epiphysis" or SCFE, S-C-F-E. This is an example of a Salter Harris Type I fracture that involves the proximal femoral growth plate and it's seen most commonly in boys that are African-American and also commonly seen in obese children. 03:42 The frontal view here demonstrates widening of the right physis. 03:47 If you compare the right versus the left, you can see that the right is actually significantly wider than the left is and it also results in displacement of the epiphysis. 03:58 So this portion of the bone right here is the epiphysis and when you compare that with the left epiphysis, you can see that it's actually been displaced medially. 04:08 So this occurs when the femoral head slips posterior and medial to the rest of the femur and it's likened to ice cream falling off of a cone. 04:16 If you take a look at the appearance, it feels like the ice cream is the epiphysis and that's falling off of the cone medially. 04:22 So an incomplete fracture is one that can occur in a soft bone and that's why it's seen most predominantly in the pediatric population. 04:28 It involves only a portion of the cortex rather than involving the entire cortex which is commonly seen in mature bones. 04:35 There are 2 major types of incomplete fractures. 04:37 There's the Torus or Buckle fracture which results in partial compression of the cortex and there's the greenstick fracture which involves only a portion of the cortex. 04:46 So let's take a look at this image here. 04:48 So we have two images of the wrist and then we have a single image of the forearm. 04:55 So what do we see here? So on this coned down image of the distal radius, we can see a very subtle fracture line that involves this portion of the cortex. 05:10 It comes partway through, but this portion of the cortex is not really involved. 05:15 We see a similar kind of fracture here of the radius. 05:21 So this is an example of a greenstick fracture or an incomplete fracture. 05:26 This involves the distal radius as seen on the wrist and we can see that it only involves one side of the cortex. 05:32 It doesn't go all the way through and this is again very commonly seen in immature bones. 05:36 And now let's take a look at this one. 05:38 This is another example of a wrist. 05:40 This is a skeletally immature patient. 05:42 We can see the growth plate open right here and you can see that the carpal bones are actually underdeveloped which is commonly seen in the pediatric population. 05:49 These become slowly more developed overtime as the kids get older. 05:53 So the abnormality is right here. 05:57 You can see a little buckling of the distal radial cortex and you can see that it kind of extends through and there's a buckling on the other side as well which is slightly more subtle. 06:07 So this is an example of a buckle or a Torus fracture of the distal radius. 06:12 Here we have a Supracondylar fracture. 06:14 So as you recall in adults, when you have a posterior fat pad sign or the presence of a fat pad posterior to the distal humerus, that would mean a radial head fracture which is very commonly seen in adults. 06:26 In kids, however, the most common elbow fracture is the supracondylar fracture, so when you see the presence of a fat density posteriorly, as delineated by this arrow, that would indicate a supracondylar fracture which can otherwise be very difficult to see. 06:40 This is the most common elbow fracture in a child and the other way of looking at it is to draw an anterior humeral line as you can see here. So the line should normally intersect the middle of the capitellum which is right here. 06:53 As you can see, this line actually intersects the anterior aspect of the capitellum, so there is slight displacement which is another way of looking for a supracondylar fracture. 07:03 So we've gone over the Salter Harris Classification which is a very commonly used classification for kid's fractures. 07:09 As you look at pediatric films in the future, keep this in mind and you can use it as a reference to describe the fractures that you are seeing.
About the Lecture
The lecture Pediatric Fractures by Hetal Verma, MD is from the course Pediatric Radiology. It contains the following chapters:
- Pediatric Fractures
- Types of Incomplete Fractures
Included Quiz Questions
Salter Harris II fractures...?
- ...have a good prognosis.
- ...are rare.
- ...enter the joint space.
- ...involve the growth plate, metaphysis, and epiphysis.
- ...have a very poor prognosis.
Which of the following is TRUE regarding the pediatric Salter-Harris classification of fractures?
- There are 5 types of fractures in the Salter-Harris classification.
- Salter-Harris type V is the least severe fracture.
- Salter-Harris type V may be occult on imaging but has a good prognosis.
- Type II fracture causes premature growth plate fusion and osteoarthritis.
- Type III is through the growth plate, metaphysis, and epiphysis.
The slipped capital femoral epiphysis is…?
- …seen most commonly in boys.
- …seen less often in African American children.
- …a type of Salter-Harris type III fracture.
- …seen on X-ray with narrowing of the joint space.
- …seen on X-ray with the femoral head displaced laterally to the rest of the femur.
Which is the most common type of elbow fracture in a child?
- Supracondylar
- Torus
- Smith
- Monteggia
- Colles fracture
Author of lecture Pediatric Fractures

Hetal Verma, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Enjoyed listening to you a lot Dr! Thank you for sharing your knowledge
