Playlist
Show Playlist
Hide Playlist
Other Dementia: Vascular Dementia

-
Slides Other Dementias.pdf
-
Download Lecture Overview
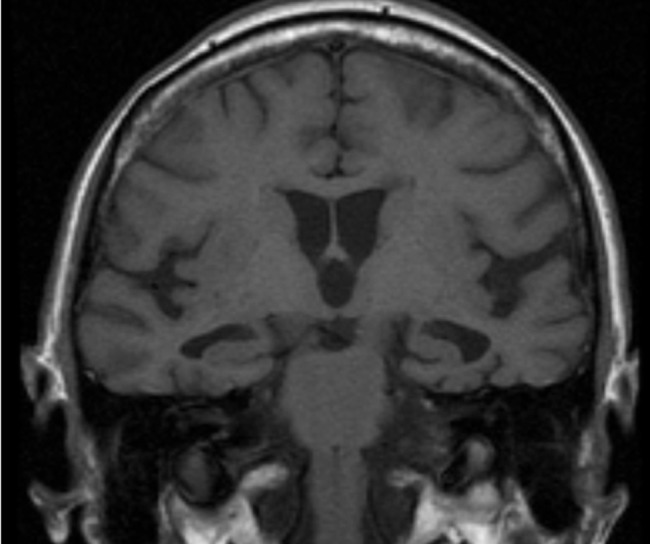
00:00 Now let's talk about vascular dementia. This is one of the most common causes of an acquired dementia. It's the second most common cause of dementia in the elderly. 00:11 It's the product of chronic ischemia and also potentially multiple acute infarcts that can occur on the brain. And the typical clinical manifestations include a decline in cognitive ability with later onset memory impairment. And there are a couple of key features that we want to hone in on. One is patients often develop a stepwise progression of symptoms as opposed to slowly progressive linear development of symptoms over time and memory impairment is often late which contrast with Alzheimer's disease where memory impairment is often early. And here, we can see a typical MRI for a patient with vascular dementia. We're looking at an axial flair of the brain and we see around the ventricles this area of T2 flare hyperintensity. 00:56 Those areas around the ventricle are the small vascular beds and with longstanding vascular disease we see damage to the small arterioles which contribute to the development of cognitive decline and dysfunction. So what's going on in the brain to contribute to vascular dementia? There are a few things I want you to remember. 01:16 First is vascular dementia results from a combination of risk factors and likely genetic variants. It's that interplay between genetic risk and environmental insults. 01:26 And there's a number of things that are happening within the blood vessels and brain that can contribute to vascular dementia. We can see white matter disease and white matter dysfunction, microinfarcts that contribute to cognitive dysfunction, large territory infarcts that can result in a prominent step of cognitive decline and subsequent brain atrophy. Some patients may experience wider spread white matter disease, other more significant large infarcts, but the final common pathway is the same and that is the onset of cognitive dysfunction slowly and step-wise over time as a result of these changes. When we think about the natural history, vascular dementia can follow several different courses. One of the most common is the multi-infarct dementia where multiple areas of large vessel arterial occlusion results in accumulation of cognitive deficits over time. After each stroke, the patient just doesn't return back to normal, and you can see that in the top curve here. Subcortical vascular dementias or large arterial strokes are not the contributor but that small vessel vascular disease is driving cognitive dysfunction tend to follow a more gradually progressive course. And then single infarct dementia can occur where a significant enlarged stroke results in substantial decline without recovery in cognitive function. And so each of these time courses and natural history would be consistent with vascular dementia but from different underlying brain pathology.
About the Lecture
The lecture Other Dementia: Vascular Dementia by Roy Strowd, MD is from the course Other Dementias.
Included Quiz Questions
What is the pathophysiology of vascular dementia?
- Chronic ischemia possibly superimposed on multiple acute infarcts, leading to progressive cognitive disease
- Accumulation of beta-amyloid plaques and tau neurofibrillary tangles, leading to progressive cognitive disease
- Accumulation of alpha-synuclein in occipital and temporal regions, leading to progressive cognitive disease
- Repetitive trauma-induced lissencephaly, leading to progressive cognitive decline
Most forms of dementia follow a progressive linear development of symptoms over time. How does vascular dementia typically present?
- Stepwise progression of symptoms
- Undulating course: "one step forward, two steps back"
- Progressive linear decline over time
- Rapid decline followed by a relative plateau of symptoms
In terms of the timing of onset of memory impairment, how can a clinician distinguish between Alzheimer disease and vascular dementia?
- In vascular dementia, memory impairment is often seen late. In Alzheimer disease, memory impairment is often seen early.
- In vascular dementia, memory impairment is often seen early. In Alzheimer disease, memory impairment is often seen late.
- They are difficult to distinguish, as both have variable-onset memory impairment.
- Both display memory impairment late in the disease course.
Which variant of vascular dementia may present as a progressive, rather than a stepwise, decline in cognitive function?
- Subcortical vascular dementia
- Single-infarct dementia
- Multi-infarct dementia
Author of lecture Other Dementia: Vascular Dementia

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
