Playlist
Show Playlist
Hide Playlist
Other Considerations for Children – Anesthesia for Children

-
17 -Anaesthesia for children.pdf
-
Download Lecture Overview
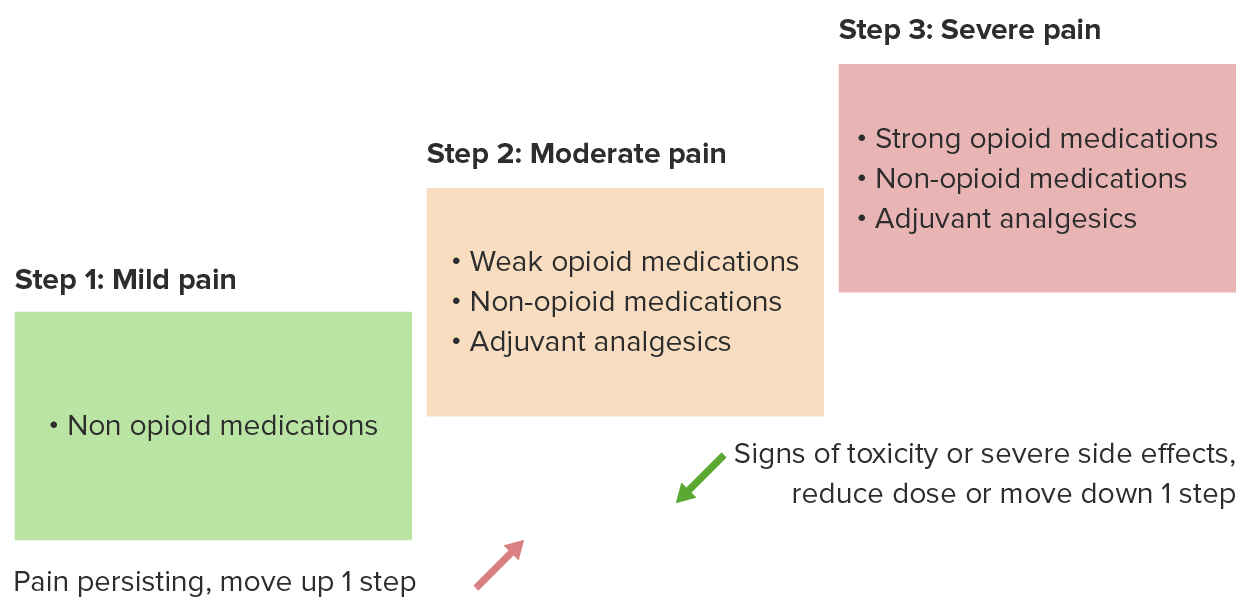
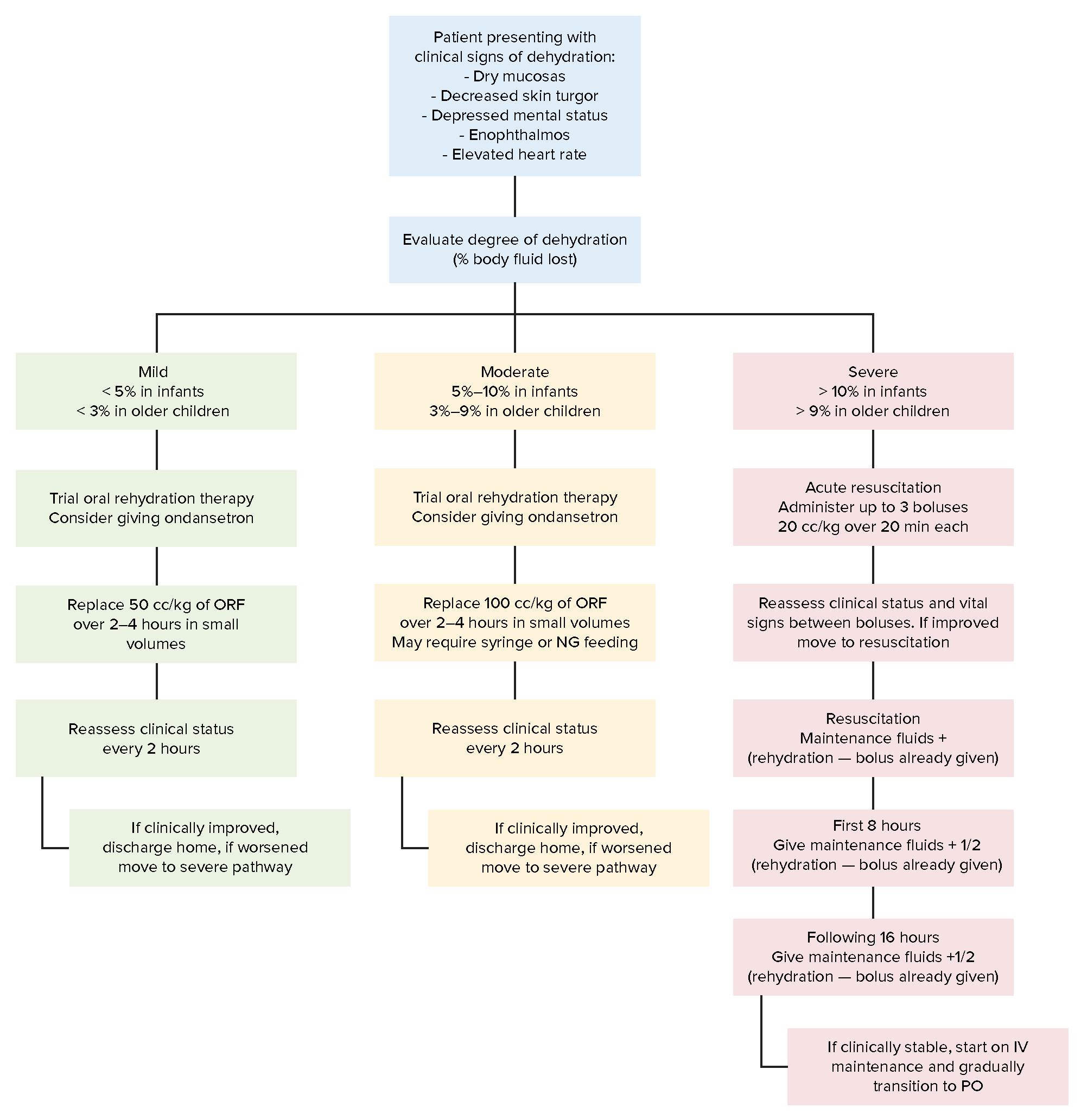
00:00 So, other considerations in pediatric anesthesia include Temperature Regulation. Children lose heat much more rapidly than adults. 00:08 And small children have trouble producing heat. They actually, newborns have something called brown fat, which is used to generate heat, where heat is generated in the rest of us and in older people, by muscle activity. So it's hard to regulate temperature in children, but it's very critical that it is regulated, because they do very poorly if they're hypothermic. 00:32 So, if you ever have to work in a pediatric operating room, you'll be surprised how hot it is, how warm it is. It's quite honestly not very comfortable and I'm glad I work in adult operating room where we all freeze, but it is very warm in the pediatric OR's to prevent heat loss. 00:50 Drug Management is much more critical. Children dosing is totally different from adult dosing and much, to many people's surprise, the actual dose of induction drug and maintenance drug required by children is proportionately much greater than that in adults. So, very small children, require quite large doses and then, as they get older, the proportional dose actually decreases. Other drugs however are totally unpredictable and you have to dose your drugs according to the child's weight or body surface area. You cannot just guesstimate how much you're going to give. 01:32 Fluid Management in children is difficult because it's extremely easy to overload a child and put them into heart failure. So you have to be skilled at this, you have to know what you're doing, and you have to pick your IV solutions and blood products very carefully. So instead of giving a unit of blood, you might only give 30 cc's of blood, or 60 cc's of blood. And you might give it slowly, and very carefully, and heated before you deliver it, in a totally different way than we do it with adults. Children often develop laryngospasm when recovering. And laryngospasm is spasm of the muscles in the larynx and in the trachea. And this can cause complete obstruction of the airway This is particularly likely to occur if you manipulate the tube when the patient's just starting to wake up, when they're still lightly anesthetized, they haven't fully recovered. If you manipulate the tube at that time it can set off a reflex that makes it very difficult to ventilate the child. It's much better to wait until the child is completely awake before you take the tube out. If they do develop laryngospasm, they tend to desaturate very quickly, because their lung capacity is very small and their oxygen demand is very high, higher than in adults. 02:56 The best way to do it, if they develop laryngospasm and they're desaturing, is to apply CPAP when you bag and mask. And CPAP just means that you maintain steady pressure at the end of expiration. And in most children, that will overcome the spasm in the larynx and cause it to open and you can ventilate quite adequately at that point. 03:20 If it doesn't work, you have to paralyze the child and consider reintubating. 03:26 As children get a little older, needle phobia is very common. The commonest age for really severe needle phobia is, in girls around 13-14, and in boys around 19 to about 24. So the boys, as one might expect, mature a little less quickly than the girls. Pain management must be customized to the personality, size and conditions of the child. They sometimes need quite large amounts of pain medications, and you have to adjust according to the needs of the child. 04:02 Anesthesiologists who provide care to premature babies or children requiring highly sophisticated surgical procedures like cardiac surgery, or neuro-surgery, burn surgery, thoracic surgery, or other highly specialized areas of surgery, the anesthesiologists require extra training. And in my country, the average pediatric anesthesiologist working in a pediatric hospital has done an additional two years of training beyond the usual five years already required for anesthesia training.
About the Lecture
The lecture Other Considerations for Children – Anesthesia for Children by Brian Warriner, MD, FRCPC is from the course Anesthesia in Special Situations.
Included Quiz Questions
What is the source of heat generation in the newborn?
- Brown fat
- Muscle activity
- White fat
- Metabolism
- Skin
What can happen when a child is extubated before the child awakens?
- Laryngospasm
- Bronchospasm
- Hypoxia
- Aspiration
- Cyanosis
What is the most important point to remember when giving IV solutions or blood products to a child?
- Fluid overload can occur easily, causing heart failure.
- Administer fluids at less than body temperature, to avoid heat stress.
- Administer fluids above body temperature, to conserve body heat.
- Withhold half of the fluids needed until the child is fully awake.
- IV solutions and blood products should not be given at the same time.
Author of lecture Other Considerations for Children – Anesthesia for Children

Brian Warriner, MD, FRCPC
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
