Playlist
Show Playlist
Hide Playlist
Opiate Receptor Agonists – Analgesics, Case Reports and Obstetrical Pain

-
16 -Analgesics case reports and obstetrical pain.pdf
-
Download Lecture Overview
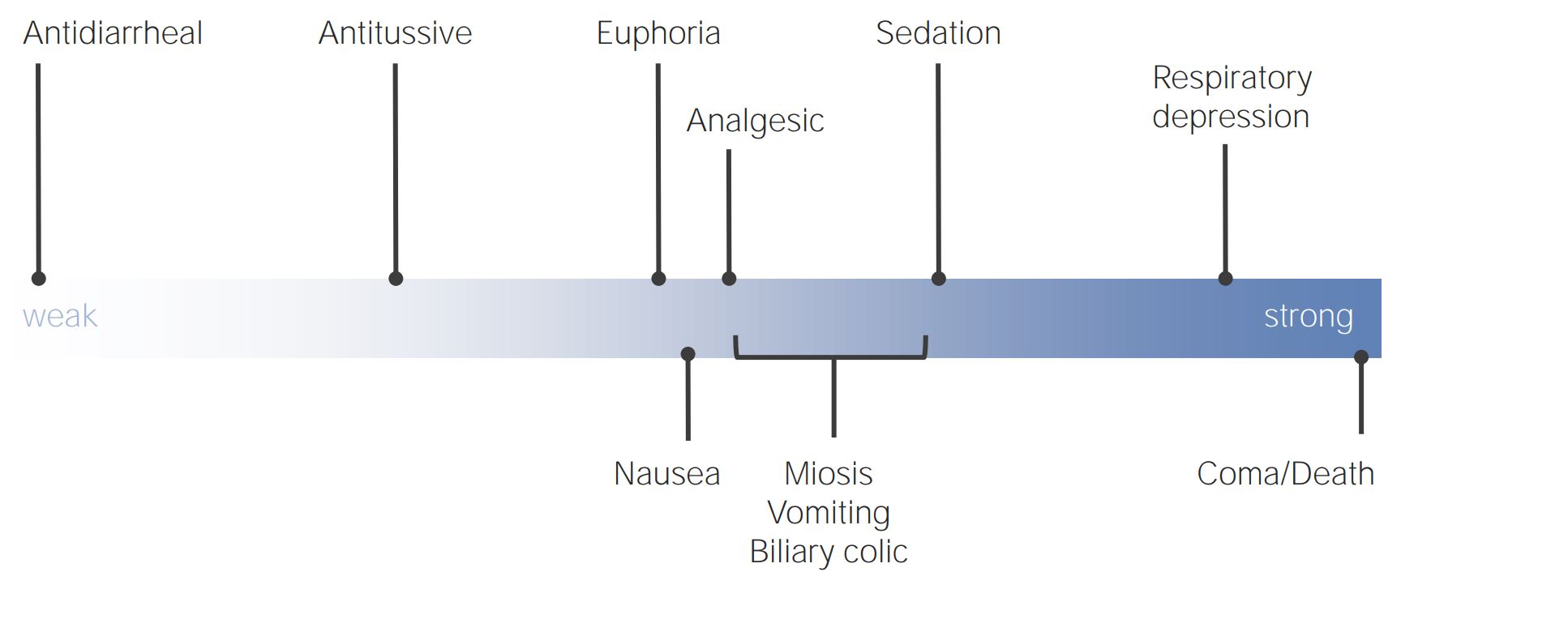
00:06 So, hello ladies and gentlemen. This is a continuation of our ongoing series of lectures on Anesthesiology. And this particular lecture is a continuation of the Management of Pain, which we started in the last lecture. We're going to spend some time in this lecture talking about the many other forms of medication that are used in management of pain. We're going to talk about three patients and how one would go about managing their pain. 00:36 And then we're going to end with a discussion of Obstetrical Analgesia and how we manage pain during obstetrical care. So, these are some of the drugs we use. And these are Classes of Drugs. 00:48 There's Opioids, which we've already talked about. Non-steroidal anti-inflammatory drugs, we've talked about. We're going to talk a little bit about Tricyclic antidepressants, Serotonin-norepinephrine reuptake inhibitors, Anti-convulsants, NMDA receptor antagonists, Alpha2 - agonists, 5HT1 - agonists for migraine, and then we're going, we've already talked about Nitrous oxide as an analgesic. We won't come back to that. So opioids, as I've mentioned, act on the mu-receptor in the brain and spinal cord to produce both effects, and unfortunately side-effects. And the side-effects are common. Respiratory depression in higher doses. Nausea and vomiting in very low doses. Constipation, extremely common. Sedation, very common. 01:36 Dizziness. Sometimes euphoria, but the majority of people have Dysphoria, which is the opposite of euphoria. Instead of feeling happy, they just feel generally lousy. Confusion, muscle rigidity, pruritus are also potential complications. These drugs are ideal for managing acute pain, but are often ineffective in chronic pain and lead to dependence, as we've talked about. We've already talked about tolerance and physical dependence. They can lead, of course, to addiction in those people who are susceptible. Remember what I said earlier, physical dependence occurs in anyone. So none of us are able to prevent ourselves becoming physically addicted to these drugs. It happens to us all. But the majority of us hate them and don't find any need to continue them once the pain is well controlled. So, once the pain is gone, we're able to stop the drugs. We go through a short phase of physical withdrawal, which may include some sweatingness, nausea and vomiting, general unpleasant feeling. 02:42 But most of us don't want to use them anymore, we don't like these drugs. Addiction occurs in those people, relatively few, who get this high or this euphoric phase from opiates. 02:54 And they become drug seekers. And they become incredibly difficult to deal with, and manage, and help. Here are a few of the drugs that are commonly seen under the Opiate banner. And I'm only going to go through this briefly just because some of them are going to surprise you, that they, actually a lot of them just turn into morphine when they're given. So Codein, which is used as, usually in very low doses as a non-prescription drug, and in higher doses as a prescription drug, is rapidly converted to morphine in the liver. So, you take it orally, it goes to the lever, it's turned into morphine. The dose of morphine is very small, but that is what causes the analgesia. 03:36 It's commonly used also as an anti cough medication, because all opiates suppress cough. 03:42 And it's a mild analgesic. I hate this drug, the side-effects are very common. 03:48 And some medical groups, including the Canadian Medical Association, have urged that it be removed from the market. 03:54 But the Canadian government hasn't caught on yet and it's still out there. Heroin, the drug which most addicts will tell you is the drug that gives them the best feeling, is also converted to morphine when it's given. There is no evidence in the therapeutic literature that heroin is a better analgesic than morphine. But addicted people will tell you that it produces more euphoria than morphine, but those studies are inconclusive. So, why do people crave heroin? We really don't know. It doesn't appear to have any particular properties that make it either superior or very different from morphine. And the active agent from heroin is morphine. Fentanyl is a drug that's now widely used for the treatment of chronic pain that was initially only used by anesthesiologists. It's a very potent drug, 100 times more potent than morphine. It has an intermediate duration. It's used by anesthesiologists, emergency physicians, intensivists intravenously, but it's used in chronic pain manager primarily in patches: percutaneous or transcutaneous fentanyl patches, can be effective in reducing chronic pain. Sufentanil, another drug in the same family, it's 1000 times more potent than morphine, it's also of intermediate duration, and it's used almost only by anesthesiologist during surgery. Remifentanil is an oddball opiate, it's 70 times as potent as morphine, but it has a half life of only one and a half minutes. 05:30 So, it's given by infusion rather than by intermittent injections. 05:36 It's also not metabolized in the liver as all other opiates are, it's metabolized by ester hydrolysis in plasma. And it's given, as I mentioned, only by continuous intravenous infusion. And I'm unaware of anybody other than anesthesiologists using this drug. 05:54 So, the good news when it comes to opioids is that, although the agonists are very complex and difficult to manage in some people, it's actually incredibly easy to reverse these drugs, using either Naloxone, which is given intravenously, has a very rapid effect, seconds before it reverses the effect of the opioid. It's given primarily by emergency physicians and anesthesiologists. 06:24 Emergency physicians tend to use fairly high doses and this can cause accelerated opium withdrawal in patients who have been addicted to the drugs. 06:36 Anesthesiologists, being a more conservative group, we tend to give very dilute Naloxone and give it in small aliquots. And this technique actually allows patients to resume respiratory activity with relatively little effect upon return of pain. So in patients, pain control remains reasonably good and they breathe, which is the goal of all of this. Naltrexone is exactly the same as Naloxone in its action, but it's longer acting and it's used in the treatment of both opioid addiction and alcoholism. And I honestly have no idea how it works in alcoholism, because there is no similarity between alcohol and opiates, either chemically or in terms of their actions on the brain. 07:24 The interesting things about Naloxone and Naltrexone is that, if they're given in the absence of opioids, they have virtually no physiological effect. So they're quite safe drugs to use and they can be used to help people who are addicted to these drugs.
About the Lecture
The lecture Opiate Receptor Agonists – Analgesics, Case Reports and Obstetrical Pain by Brian Warriner, MD, FRCPC is from the course Anesthesia.
Included Quiz Questions
Which of the following receptors do opioid receptor AGONISTS act on?
- Mu receptor
- Alpha receptor
- Kappa receptor
- Beta receptor
- NMDA receptor
Which of the following is the MOST commonly encountered side effect of opioid receptor agonists?
- Sedation
- Nausea
- Vomiting
- Respiratory depression
- Dysphoria
Which of the following clinical symptoms would opioids be ideal to use for management?
- Acute pain
- Chronic pain
- Preoperative pain
- Cough
- Constipation
Which of the following drugs is NOT metabolized by the liver?
- Remifentanil
- Heroin
- Morphine
- Fentanyl
- Oxycodone
Author of lecture Opiate Receptor Agonists – Analgesics, Case Reports and Obstetrical Pain

Brian Warriner, MD, FRCPC
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
