Playlist
Show Playlist
Hide Playlist
Obstetrical Pain – Analgesics, Case Reports and Obstetrical Pain

-
16 -Analgesics case reports and obstetrical pain.pdf
-
Download Lecture Overview
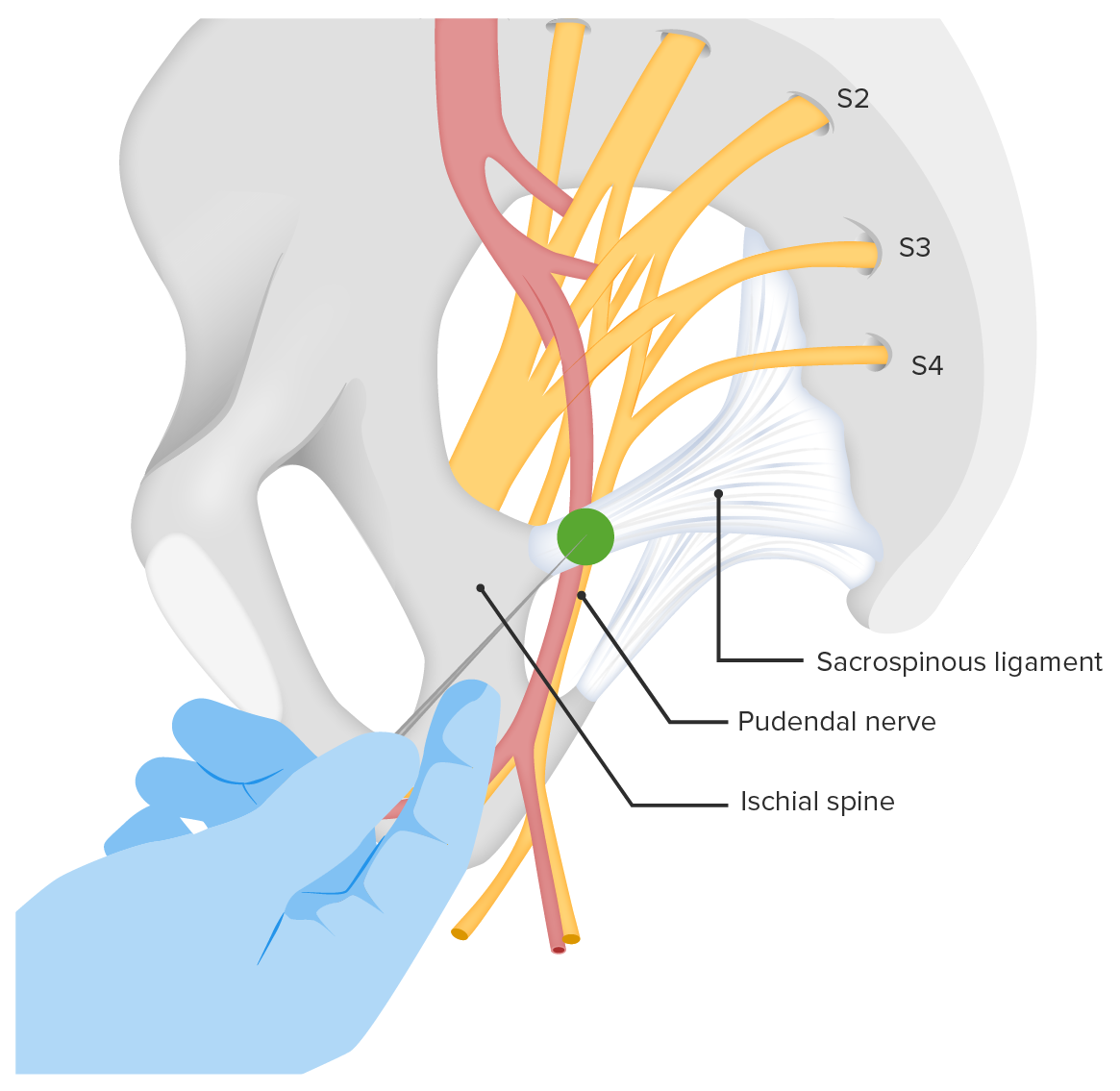
00:00 So, we're going to move over to another area completely. This is the treatment of obstetric pain. And the reason that I place obstetric pain separate from acute pain or from chronic pain is that, it truly is unique. 00:14 It's the only condition in humans that results in intermittent, very severe pain, and intermittent periods of relaxation and loss of pain. 00:26 It's really quite unique. It can be very intense, but unlike most pain, it's intermittent. When we provide pain relief, we have to take into account the fact that it's intermittent pain. And we must also take into account that we're dealing with a mother and a baby. And that anything that we provide to mom, may very well make it to baby and may not be a good thing for baby to receive. So, there are two areas of innovation for the uterus that come into play during labour and delivery. The first occurs in segments T10, thoracic 10, to the first lumber segment. And this is the pain that women feel during actual labour. This is the abdominal pain they feel. 01:14 And it, as we've already mentioned, is intermittent, severe, and it tends to become more severe as labour goes on. So, it starts with a few fairly mild little pains, and then it slowly builds up over time and becomes extremely intense. The pain of delivery is served by nerves from S2, Sacral 2 to Sacral 4. And this is pain in the perineum area of the body. It's also intermittent and is related to the labour pain, to the contraction of the uterus, but it's a different kind of pain and it tends to occur later in the labour phase. So in early labour, the pain is largely in the abdomen, above the pubis. And epidural analgesia works like a dream. And you use low concentrations, you can completely remove the sensation of pain, but the woman will often continue to be aware that she's contracting and that's the ideal situation. However, in late labour the pain spreads over the entire abdomen and into the perineum, and becomes much more severe. And at that point, we use higher concentrations of local anesthetic in the epidural to provide pain relief in that area. The local anesthetics are not transferred across the placenta to the baby. So there's no concern about fetal toxicity from local anesthetics. However, opiates are transferred to the baby. 02:44 So, we usually have very low doses of opiates included in our epidural, but you must be very careful not to rise with the pain, rise the opiate level, because that is transmitted to the baby and it may cause respiratory depression in the newborn. 03:02 There are lots of other modes of obstetric pain relief. But I can say with some certainty that nothing works as well as epidurals. But other conditions such as, or other modes such as psycho-prophylaxis, which is usually mom plus her partner working on breathing, certainly can help in the earlier stages of labour. And certainly, mom and the partner, dad in many cases, feel like they're participating in something together and they can work as a team. Massage, baths and acupuncture have all been used to varying degrees of success. Nitrous oxide, which is breathe through a demand valve, so it only goes to the patient when she takes a breath in, is also used. So, the patient has to be taught how to use it. She has to be told that as soon as she starts to feel the contraction developing, she should take a big breath of nitrous oxide or a couple of breaths. And this will produce quite effective analgesia, but only of intermediate potency. So later in the labour it's probably not going to be terribly useful. Can cause sedation and confusion. And it should never be delivered by the partner. In other words, if mom's lying there and contracting, the husband should not put the mask on and hold it in place. It's important that the patient control it, takes her breaths and drops the mask so she doesn't have an overdose of the nitrous oxide. Intravenous narcotics are sometimes given, but remember what I said, they do transfer to the baby and there's a potential for respiratory depression in the newborn. Ketamine is used primarily, if it's used at all, early in labour in small doses. 04:50 And it produces good analgesia, it is transferred to the baby, so you can have a baby that's anesthetized and you don't want that. So it's only used early in labour and in very small doses. 05:02 And intramuscular narcotics have been used. They're not effective, generally because they don't, they're not absorbed quickly enough to be effective. But they're longer lasting, they do go to the baby and they can cause all the problems in the baby that you just don't want to see. So the goal of obstetric analgesia is to provide the patient with as much comfort as possible without affecting the fetus. 05:26 Many drugs can cross the placenta and have an effect upon the baby, but local anesthetics, asI've mentioned, do not. Care must be given when opiates are given because they do cross. And labour, the good news, is labour is not delayed by epidural analgesia, nor is the rate of C-section increased by epidural labour analgesia. 05:50 These are both statements that are commonly made and there's a vast amount of evidence that says that they're simply incorrect. That labour is not affected, nor is a C-section rate affected. So this is the International Association for the Study of Pain. If you have further interest in this subject, you should look at this website. It's a very good website. So in summary, in this lecture we've talked about a number of drugs that are used in the management of pain, both their usefulness and their side-effects. We've had three very short case presentations. 06:26 And an appreciation, I hope, of how pain is managed in different conditions. And we've ended with that unique form of pain, obstetrical pain, and how we use epidural and other forms of pain management to safely care for the mother and for the baby.
About the Lecture
The lecture Obstetrical Pain – Analgesics, Case Reports and Obstetrical Pain by Brian Warriner, MD, FRCPC is from the course Anesthesia.
Included Quiz Questions
Which spinal cord segments provide the nerve supply to the uterus?
- T10–L1
- T10–L5
- T9–S2
- L2–L5
- S2–S5
What is the management plan for pain in late labor?
- Use a higher concentration of local anesthetic.
- Use a lower concentration of local anesthetic.
- Do not use anesthetic.
- Administer an analgesic.
- Administer both an analgesic and anesthesia.
Why is local anesthesia preferred for pregnant women during labor?
- It cannot cross the placenta.
- It can cross the placenta.
- It is safe for the mother.
- It is easier to administer.
- It is safer for anxious individuals.
Author of lecture Obstetrical Pain – Analgesics, Case Reports and Obstetrical Pain

Brian Warriner, MD, FRCPC
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
extremely thankful prof. you cleared many concepts of pain managment
