Playlist
Show Playlist
Hide Playlist
Neuromuscular Blockers – Skeletal Muscle Relaxants

-
Slides Neuromuscular Blockers Skeletal Muscle Relaxants.pdf
-
Reference List Pharmacology.pdf
-
Download Lecture Overview
00:01 The depolarizing agent that we use in human is succinylcholine. Now what is succinylcholine? Succinylcholine is two acetylcholine molecules linked together end-to-end. 00:13 The onset of action of succinylcholine is about 1 minute, and the duration of action is 6 to 11 minutes. 00:19 It does have side effect though. It can cause post op muscle pain. It can cause hyperkalemia because you're spilling potassium into interstitial tissues. And it can cause gastroesophageal reflux disease and aspiration because the muscles in the smooth muscles in stomach will contract. 00:40 Important drug interactions. Succinylcholine can interact with inhaled anesthetics to cause malignant hyperthermia. 00:47 Remember, I discussed this in a previous lecture, the antidote to malignant hyperthermia is dantrolene. 00:55 And I've said this before, malignant hyperthermia, dantrolene, under one minute. 01:01 Isoflurane and other inhaled anesthetics can also potentiate neuromuscular blockade. 01:07 So this is something that we have to keep in mind, when we're administrating anesthetic drugs. 01:12 Now, aminoglycoside antibiotics will also interact with succinylcholine. 01:17 Gentamycin, tobramycin, these may potentiate skeletal muscles relaxants. 01:24 Remember that succinylcholine is not reversed with the cholinesterase inhibitors like pyridostigmine. 01:33 Now, let's think about that, why? Well, pyridostigmine is a cholinesterase inhibitor. 01:39 What it does is it leaves more acetylcholine in the synaptic cleft. When you have succinylcholine, that acetylcholine is going through the channel, and the muscle is already depolarized. 01:52 Adding more acetylcholine is not going to solve the problem. 01:57 You have to be cautious with these agents. We want to be careful with succinylcholine in our older patients. 02:04 We want to be careful with patients who have had previous myastenia gravis because their acetylcholine receptors are a bit damaged. And you have to be careful of people who have genetic variants that metabolize succinylcholine very slowly. They will have a prolonged response. 02:21 The other caution that I'm going to put out there is hyperkalemia. 02:24 Remember that when you have succinylcholine administered to a patient, you're going to depolarize the muscle and you may release potassium. It's particularly bad in burn victims because they have been burned, they have lots of cellular damage, and all of those cells have released potassium into the blood. 02:43 In upper motor neuron disease, remember that these are muscles that are not normally contracting, or spinal cord injury, it's the same thing, so when you contract those muscles or you depolarize those muscles, you will release a lot of potassium. And finally, patients who have intra-abdominal infection also are hyperkalemic in response to succinylcholine. We believe that this may be due to damage to cells as well, but we're not entirely sure of the mechanism in this case. 03:11 Let's take a look now at the non-depolarizing agents. Now, we have got a large list there, let's just separate them out in terms of how long they act, or how quickly they act. 03:24 Let's start with rocuronium. Rocuronium is used as a very important neuromuscular blocker in anesthesia and we sometimes use it in the intensive care unit as well when we want to paralyze patients as we have them on ventilators. 03:38 It is eliminated through the bile. The onset of action is about one to two minutes, with a duration of ation of 35-75 minutes. 03:47 I personally have more experience with pancuronium. This is something that is used in the ICU. 03:53 It has an onset of action of about 3 to 4 minutes, with a duration of action of 35 to 75 minutes and lasts for about 35 minutes. 04:02 Finally, there is tubocurarine. Tubocurarine has an onset of about 3 to 6 minutes, and lasts about 60 to 120 minutes. It is no longer available in the USA. It is eliminated through the kidney. It's a prototypical drug, but it is derived from curare which is a naturally occuring paralytic that was first found in Amazon tribes which is a naturally occuring paralytic that was first found in Amazon tribes who used to tip their arrows with this deadly agent. 04:29 Okay. With respect to these agents, they can be reversed with cholinesterase inhibitors which increase the level of acetylcholine in the synaptic cleft. 04:40 That is different from the depolarizing agent succinylcholine. There is also a chemical antagonist of rocuronium called sugammadex, which directly binds to this steroid-based NMBA, forming a complex that prevents the NMBA from acting at the neuromuscular junction. 04:57 Here's a summary slide about the Neuromuscular Blocking Agents that were discussed: For succinylcholine, the onset of action is approximately 1 minute. This rapid onset makes succinylcholine ideal for situations requiring quick muscle relaxation, such as rapid sequence intubation. 05:15 The duration of action is 6-11 minutes, which is short due to the rapid hydrolysis by plasma butyrylcholinesterase, also known as pseudocholinesterase. It is primarily broken down by plasma butyrylcholinesterase. Its fast metabolism contributes to its short duration, making it the drug of choice for short procedures. 05:37 The onset of action of Rocuronium ranges from 1-2 minutes, making it one of the faster-acting non-depolarizing agents. 05:45 Its duration of action is between 35-75 minutes, which allows for longer procedures without the need for frequent re-dosing. 05:54 It is eliminated primarily by the liver, which means its action may be prolonged in liver dysfunction. 06:01 For Pancuronium, the onset of action is 3-4 minutes. While not as fast as succinylcholine or rocuronium, it's useful for longer procedures. Its duration of action extends from 85-100 minutes, providing a long duration of muscle relaxation. 06:18 It is eliminated mainly through the kidneys (80%), so its elimination and duration can be significantly affected in renal impairment. 06:27 D-tubocurarine is not available in the USA currently but is important historically and for comparative purposes. 06:34 Its onset of action is between 3-6 minutes. This slower onset limits its use for emergency intubation. 06:42 Its duration of action ranges from 60-120 minutes, which is a prolonged duration requiring careful monitoring. 06:50 Its elimination is primarily by the kidneys, so renal dysfunction can prolong its effects. 06:55 Remember that the choice of an NMBA should be tailored to the patient's medical history, the surgery type, and the expected duration.
About the Lecture
The lecture Neuromuscular Blockers – Skeletal Muscle Relaxants by Pravin Shukle, MD is from the course CNS - Pharmacology. It contains the following chapters:
- Depolarizing Neuromuscular Blockers
- Nondepolarizing Neuromuscular Blockers
Included Quiz Questions
Succinylcholine is best characterized as...?
- ...a depolarizing neuromuscular blocking agent.
- ...a spasmolytic agent used for chronic back pain.
- ...a non-specific neuromuscular blocking agent.
- ...an anti-anxiety medication with muscle relaxant properties.
- ...a reversible acetylcholinesterase inhibitor used in Alzheimer treatment.
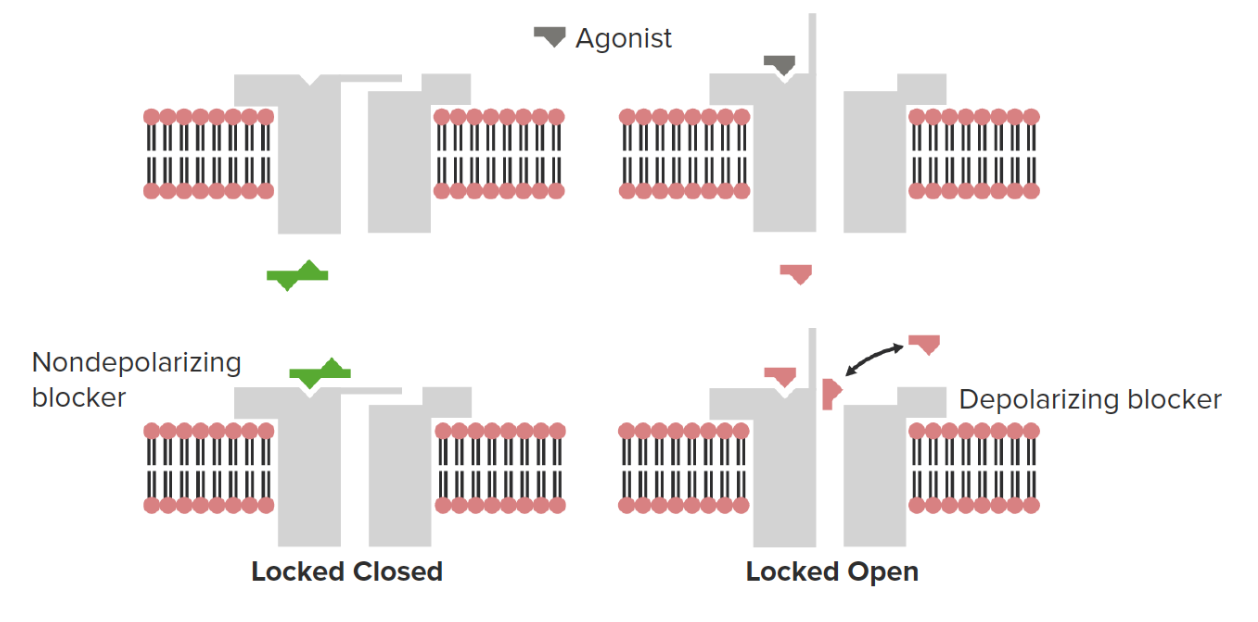
What is the effect of a non-depolarizing neuromuscular blocker on the ion channel gate at the neuromuscular junction?
- The gate will be closed.
- The gate will remain permanently open.
- The gate's permeability to calcium ions increases.
- The gate will oscillate rapidly between open and closed states.
- The gate's selectivity for potassium ions over sodium ions is enhanced.
Author of lecture Neuromuscular Blockers – Skeletal Muscle Relaxants

Pravin Shukle, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
