Playlist
Show Playlist
Hide Playlist
Myelopathy – Vascular Disorders with Case

-
Slides Diseases of the Spinal Cord.pdf
-
Download Lecture Overview
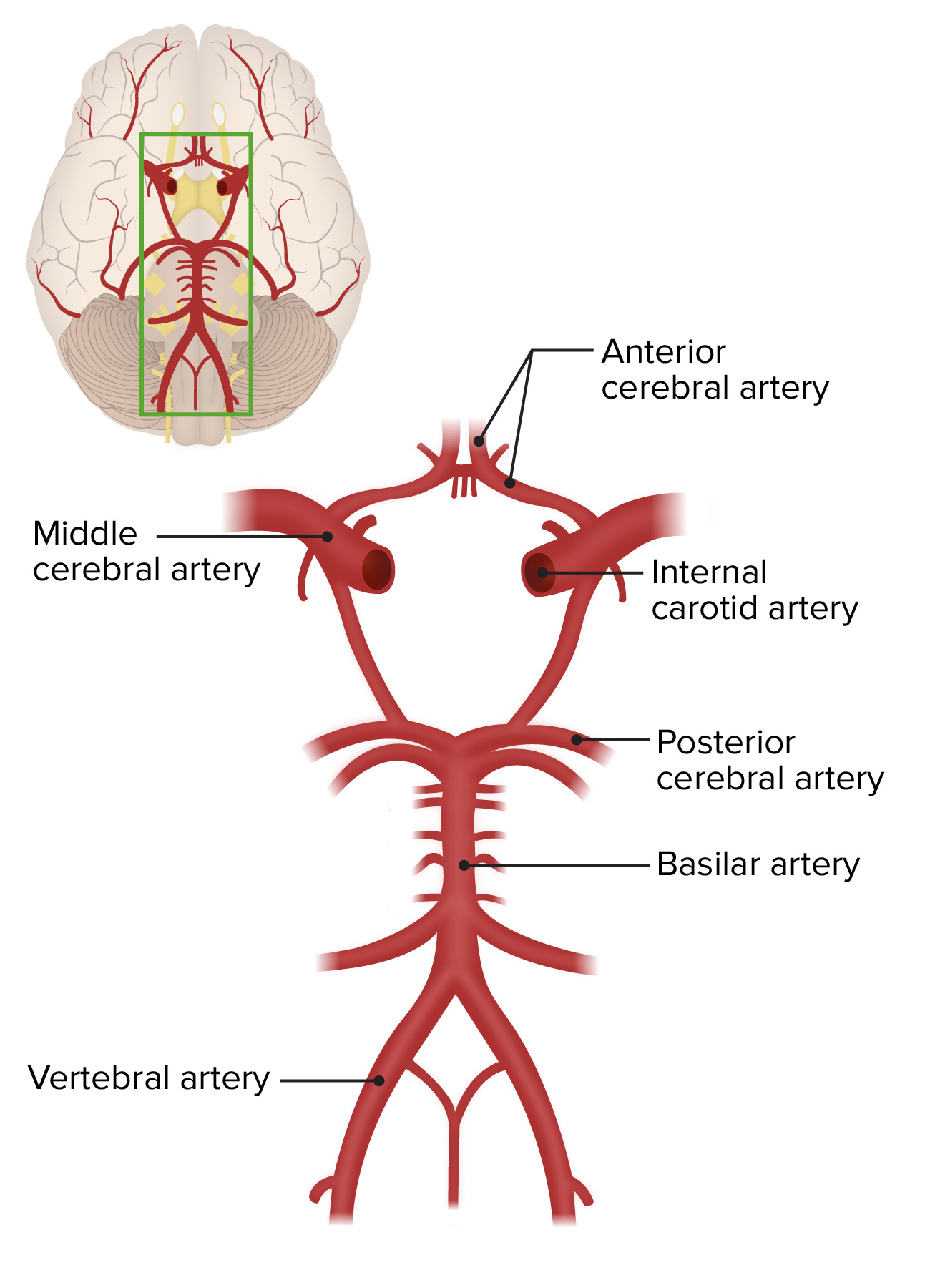
00:00 Now, let's look at some of the vascular disorders that affect the spinal cord and talk about vascular myelopathy. And let's first turn to a case. This is a 78-year-old who presents as a transfer for acute onset of bilateral lower extremity weakness. Acute onset, anything, should make us think of a stroke or a vascular lesion so already we're concerned about that type of pathology. She was admitted to an outside facility with infrarenal aneurysm and underwent repair with endograft replacement. 00:32 Postoperatively, she was found to have weakness in the right more than left leg with numbness, bowel and bladder problems. She was unable to initiate urination, had incontinence and bladder fullness. The patient has chronic low back pain that is not different from previous. And so pain isn't a prominent part of this presentation but an acute paraparesis or acute myelopathy appears to be the case. Examination shows 1/5 strength in the bilateral lower extremities and normal upper extremity strength that's consistent with a paraparesis and that should point us squarely to spinal cord pathology. Deep tendon reflexes are 1+ in the upper extremities and trace in the lower extremities with mute plantar responses, which is different than what we would normally see. Typically, with spinal cord disorders we expect hyperreflexia. 01:19 But in the acute setting and particularly in the setting of spinal cord shock, we can see a transient or temporary period of hypo or even areflexia in those patients and this trace lower extremity reflexes are consistent with an acute cord injury. 01:35 Sensation is impaired to touch at L4, L5 and S3 dermatomes on the right side and vibration and proprioception appear intact. So we're seeing some asymmetry in the types of sensory findings that we see in this patient. Pain and temperature is impaired. 01:49 Vibration and proprioception are intact, which is going to become very important in differentiating the type of disorder for this patient. So let's look at some of the key features in this case. The patient has an asymmetric strength exam consistent with a paraparesis. The reflexes are different than what we would classically associate with a spinal cord disorder or myelopathy, but maybe consistent with myelopathy in this patient with an acute presentation where we may be dealing with an acute cord injury and specifically a stroke. And the sensory exam suggests that there is a certain area or region of the spinal cord that's affected. We have motor symptoms, anterolateral pain and temperature symptoms, and sparing of the dorsal columns. 02:31 And that is an important wildcard in this case. Sparing of vibration and proprioception is really going to a point to the precise etiology of this patient's presentation. This patient underwent an MRI and we see the typical finding here. We see a cross section of the thoracic spinal cord and there is increased signal just in the gray matter structures of the spinal cord in this thoracic segment, what's so called the owl eye sign. And you can see almost the appearance of the owl's eyes within the spinal cord. 03:03 The gray matter is the cell bodies. That's what's doing the work of the nerves and those are most susceptible to reduced perfusion and so this is the finding that we see in patients who present with an acute cord infarct. So let's look a little bit closer at spinal cord vascular anatomy, which is important in this case and talk about the presentation of an acute spinal cord infarct, which this patient was suffering from. 03:30 When we think about the arterial and venous supply to the cord, first we can start with the arteries and the arterial supply. The spinal cord is primarily supplied by an anterior spinal artery which is critical, and we'll talk more about that in a few slides. 03:44 There are also 2 posterior spinal arteries which are redundant and help to provide rich collaterals to the posterior aspect or dorsal aspect of the cord. And spinal branches that also give the cord arterial blood. In terms of the venous drainage, we have primarily venous drainage to the epidural venous plexus and then to the major veins that drain the body at the various segments of the spinal cord. So let's look at that here in this schematic and we're looking at the arterial supply of blood to the spinal cord. Blood supply begins up in the brain at the basilar artery and descends down in the regions of the posterior inferior cerebellar arteries and the vertebrals. Both vertebral arteries typically give off a branch that comes together to form the anterior spinal artery and you can see that depicted in this part of this schematic here and the anterior spinal artery is critical for providing blood flow to about 3/4 of the spinal cord. In addition, we have 2 posterior spinal arteries that provide rich collaterals to the dorsal aspect of the spinal cord and medullary arteries. 04:52 These are branches off the descending aorta and there are certain areas and segments where there is a large and particularly dominant medullary artery, one of those is the artery of Adamkiewicz around the T10 area and this helps to provide arterial supply to the spinal cord as it descends all the way down the body. 05:10 We can also look at this in cross section and here we're looking at a representative cross section where we have the anterior spinal artery on the ventral aspect of the cord and there are 2 posterior spinal arteries on the posterior aspect and you can see where the collaterals arise from the anterior and posterior arteries. And here we see a sulcal artery, the anterior spinal artery, and the vasocorona. Importantly, when we think about that arterial supply to the cord, there are 2 major regions that differ in their arterial supply. One is the dorsal columns and then the rest of the spinal cord. The dominant area of the spinal cord, the ventral cord and the lateral aspects of the cord are supplied by the anterior spinal artery. That's the motor descending tracts, the cell bodies of the ventral horns, and the anterolateral pain and temperature system. And so patients that present with strokes or pathology affecting the anterospinal artery will be weak, they'll have problems with pain and temperature sensation, and have a paraparesis but spare the dorsal columns. 06:22 They will have intact vibration and proprioception which is the presentation that is diagnostic of an anterior spinal artery stroke or anterior spinal artery syndrome. 06:33 The posterior spinal arteries are redundant and provide vascular supply to the dorsal columns which again is carrying information for vibration and proprioception. 06:45 In terms of venous drainage, we can see the key aspects of venous drainage of the spinal cord. There is drainage to the epidural venous plexus and then through a spinal vein to intervertebral veins and then ultimately to the azygos and hemiazygos veins to drain back towards the heart.
About the Lecture
The lecture Myelopathy – Vascular Disorders with Case by Roy Strowd, MD is from the course Diseases of the Spinal Cord.
Included Quiz Questions
Which of the following describes the "owl-eyes" sign on an MRI of the spinal cord?
- Increased signal in the gray matter structure of the spinal cord
- Increased signal in the white matter structure of the spinal cord
- Decreased signal in the gray matter structure of the spinal cord
- Alternating signal intensities in the spinal cord's gray matter and white matter
- Two empty spaces in the spinal cord
What structure of the spinal cord is most susceptible to reduced perfusion?
- Gray matter
- White matter
- Dorsal root ganglion
- Ventral root of the spinal cord
- Cervical nerve roots
What arteries do the anterior spinal arteries arise from?
- Vertebral arteries
- Basilar arteries
- Posterior inferior cerebellar arteries
- Posterior cerebral arteries
- Middle cerebral arteries
Which artery supplies three-fourths of the spinal cord?
- Anterior spinal artery
- Posterior spinal arteries
- Vertebral arteries
- Epidural arteries
- Carotid arteries
What artery is most likely affected in a patient with loss of motor function and pain/temperature sensitivity, but with relative sparing of proprioception and vibratory sense below the level of the lesion?
- Anterior spinal artery
- Two posterior spinal arteries
- Artery of Adamkiewicz
- Descending aorta
- Carotid artery
A 60-year-old man presents with paraparesis and reports he has lost awareness about the location of his arms. What artery is most likely affected?
- Posterior spinal artery
- Anterior spinal artery
- Basilar artery
- Artery of Adamkiewicz
- Carotid artery
Author of lecture Myelopathy – Vascular Disorders with Case

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
