Playlist
Show Playlist
Hide Playlist
Muscular Dystrophy in Children

-
Slides MuscularDystrophy Pediatrics.pdf
-
Download Lecture Overview
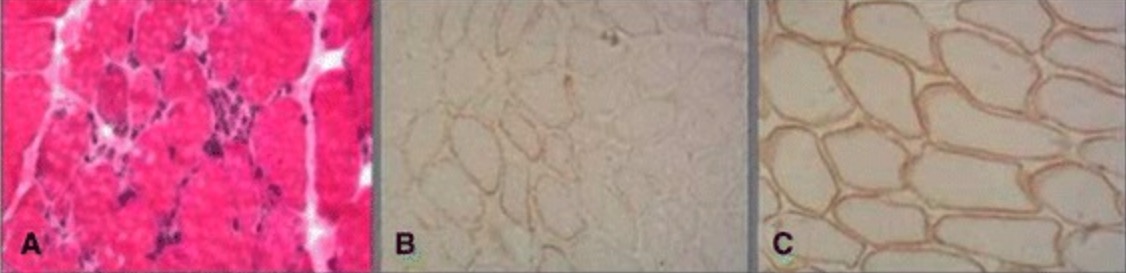
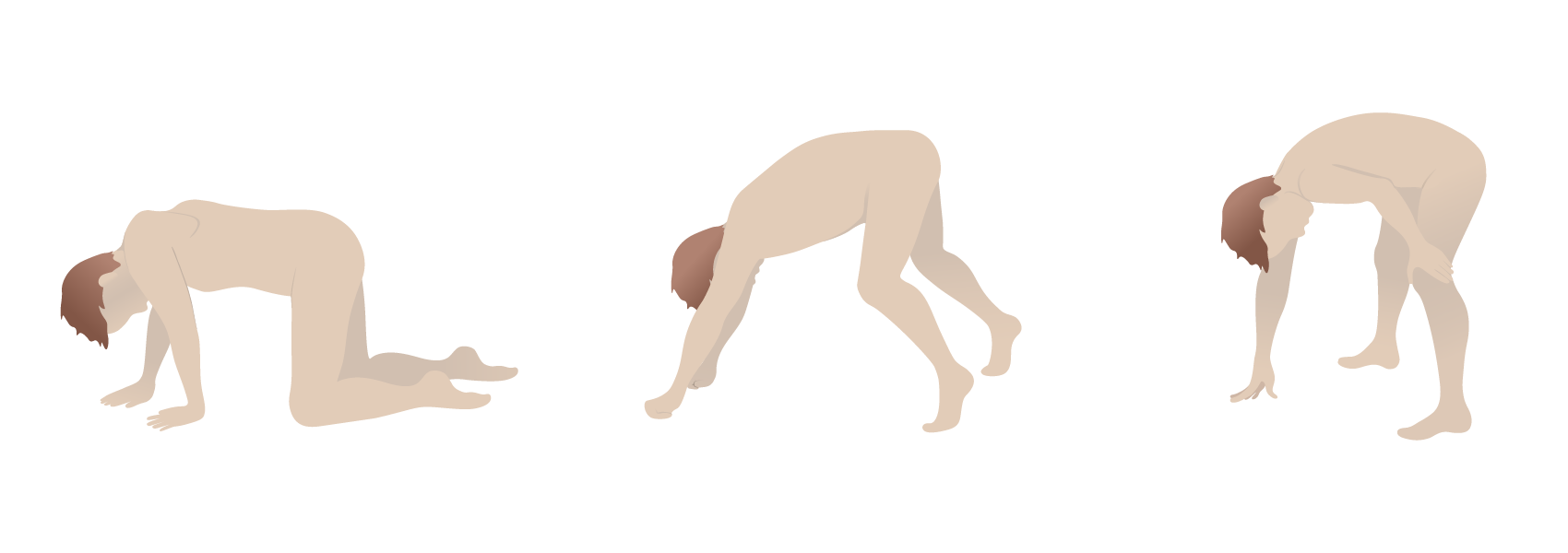
00:01 In this lecture were going to discuss Muscular Dystrophy in Children. 00:07 Muscular Dystrophies are a whole family of different disorders. 00:12 They are all dysfunctional proteins in muscle fibers and specifically problems on Dystrophin gene So, the most common type of muscle dystrophy we will talk about is Duschenne's muscle dystrophy. 00:26 There is also a slightly less, and perhaps less severe disease called Becker's muscular dystrophy And this is the two that you hear about the most. 00:35 And there are a whole family of dystrophies. 00:39 There is Myotonic dystrophy, Limb-girdle muscular dystrophy. 00:43 Fascioscapulohumeral muscular dystrophy Emery-Dreifuss muscular dystrophy Fukuyama muscular dystrophy Oculopharyngeal muscular dystrophy. 00:53 The point is there are lots of different kinds. 00:55 The one's that you should focus though are on Duchenne's and on Beckers. 01:01 So, let's talk a little bit about the dystrophin protein. 01:05 The dystrophin protein is one of the largest genes in the human genome. 01:12 When that is abnormal, patients develop muscular dystrophy. 01:16 So, let's focus particularly on Duchenne's. 01:20 Duschenne's is an X-linked disease. And that it almost entirely affects males. 01:27 This is s a devastating condition. 01:30 It affects 1 in 3,500 births. So, it is reasonably common. 01:35 And it is commonly caused by new mutations. 01:38 It will be very unusual for a patient with Duchenne's to father a child. 01:44 So in muscular dystrophy, symptoms typically start around three years of age. 01:50 Patients, children will develop abrnormal gait. 01:54 And will start having pronounced muscle weakness. 01:57 They will develop Pseudohypertrophy Pseudohpertroohy is when the muscle is large but it is weak. 02:05 and they will develop gradual muscle wasting as these muscles decline. 02:12 This is Gower's sign. 02:14 This has a high likelihood of showing up on an exam. 02:17 Typically, children will get up and they will need to use their arms to get themselves up off the floor. 02:24 This is because the primary muscles of weeknesses in muscle dystrophy and in Duchenne's are the large trunkal muscle groups such as the buttocks the thighs and the abdominal musculature So, these children will literally walk themselves up their own legs to be able to stand up. 02:42 This is pathognomonic for muscular dystrophy and almost all of them do this as part of one of their initial presentations. 02:49 because it is only recent that they were actually walking when the symptoms starts rearing its ugly head. 02:56 Diagnosis is essentially clinical. 02:59 When you see proximal muscle weakness in a young boy. 03:02 Especially a 3 year old boy, this is often the diagnosis. 03:06 Additionally, important lab findings are muscle breakdown Patients will have a very elevated CK or creatine kinase. 03:16 This is because that protein is extruded by the muscle as it degenerates. 03:20 Patients will have an increased aldolase again, extured by the muscles as they degenerate. 03:26 In patients with Duchenne's, they may have bumped Liver Function Tests as well slightly elevated ALT and AST. 03:34 The diagnosis if it must be made is made by dystrophin gene testing. 03:39 We can now sequence the gene and determine what the problem is. 03:44 Treatment for patients with Duchenne's Muscular Dystrophy is tragically, only supportive. 03:50 Where there is no cure right now for this disease. 03:53 Steroids may slow the rate of muscle degradation but the problem is the long term effects of steroids are so severe that in most cases, we choose not to use steroids. 04:05 As many of the patients in their declining years or adolescence, they can actually help you guide how you want to manage their situation. 04:13 We do give patients oral creatine daily. 04:17 Because that can improve muscle strength in patients with Duchenne's But keep in mind, that doesn't help with Beckers, which we will talk about next. 04:25 So, in Duchenne's muscular dystrophy a lot of some specialty assistance is needed. 04:33 We need to fix them with braces often as their teeth will grow abnormally. 04:39 Often these patients will require Scoliosis surgery. 04:42 Their spine will bend as the result of the promixal muscle weakness. 04:46 So orthopedists are intimately involved in their care. 04:50 Patients will eventually have difficulty with eating. 04:54 And as not being able to eat and not being able to feed is an essentially painful experience we often end up putting G-tubes in these patients so they can remain satiated as they are degenerating. 05:09 Patients often have pulmonary disease. As they get older, and they are less able to take deep breaths, we will be following them with Pulmonary Function testing and often pumonologists are involved to try and mitigate some of those respiratory symptoms. 05:23 They will be having ineffective cough for example. 05:26 And so mucolytics and respiratory toilet may be indicated. 05:31 Finally, the heart muscle is unfortunately also involved in these patients. 05:37 Patients with Duchenne's often get a cardio myopathy So, cardiologist involvement is important to continue to monitor their cardiac output and provide medications that can mitigate this problem. 05:51 Typically, the course of Duchenne's muscular dystrophy is inexorable and declining. 05:57 They typically lose the ability to ambulate entirely by 7-13 years of age. 06:03 And then they suffer a gradual respiratory failure. 06:08 These patients develop a dilated cardiomyopathy and that myopathy can cause shortness of breath congestive heart failure, and other symptoms. 06:19 One of the questions that comes up and every case must be handled differently, is whether or not to place a Tracheostomy. 06:27 Tracheostomy will prolong life but it will not always prolong the quality of life. 06:32 And involving a party of care expert maybe necessary to help guide these conversations in terms of what is the best next step for patients. 06:42 Early death in patients with Duchenne's muscular dystrophy is inevitable. 06:48 They usually die from cardiac or respiratory failure. 06:51 And the average age of death is around 16-20 years old. 06:57 Let's switch to Becker's muscular dystrophy. 07:02 In Becker's muscular dystrophy. 07:04 This is also a genetic mutation in the dystrophin gene. 07:10 It is an X-linked mutation again. And so, this is almost entirely once again occurs on boys. 07:17 This is a much milder course fortunately in Duchenne's And rarely, extremely mild with only cramping. 07:24 And otherwise a fully functional individual. 07:27 The age of onset is often later than in Duchenne's And they typically ambulate even to adolescence. 07:36 At this point ambulation becomes too hard. 07:39 Patients with Becker's muscular dsytrophy also die young but live a lot longer than patients with Duchenne's. 07:46 The average age of death is 42, plus or minus 16 years. 07:51 That is a brief summary of Becker and Duchenne's muscular dystrophy Thank for your attention.
About the Lecture
The lecture Muscular Dystrophy in Children by Brian Alverson, MD is from the course Pediatric Neurology. It contains the following chapters:
- Different Types of Muscular Dystrophy
- Duchenne Muscular Dystrophy
- Management of Duchenne Muscular Dystrophy
- Becker's Muscular Dystrophy
Included Quiz Questions
A 3-year-old girl presents with progressive generalized weakness. Her mother notices that when she stands up, she uses her arms to push up her body and has a hard time when walking. She also mentions the child has gotten "thinner." On physical examination, you notice some muscle wasting and pseudohypertrophy of calves. Which of the following is not consistent with the diagnosis of Duchenne muscular dystrophy?
- Female sex
- Gower’s sign
- Age of onset
- Abnormal gait
- Muscle wasting
Which protein is involved in muscular dystrophy?
- Dystrophin
- Myosin
- Actin
- Myelin
- Motilin
Which lab results would be seen in Duchenne's muscular dystrophy?
- Very elevated creatinine kinase
- Decreased aldolase
- Decreased LFTs
- Elevated serum urea
- Decreased alkaline phosphatase
Which of the following interventions is NOT encouraged in Duchenne's muscular dystrophy?
- High-intensity exercise
- Oral creatine
- Scoliosis surgery
- Braces for teeth
- Cardiologist evaluation
Which of the following statements about Becker’s muscular dystrophy is TRUE?
- It is an X-linked mutation.
- It is more severe as compared to Duchenne's.
- It has an early age of onset than Duchenne's.
- Muscle weakness is more severe.
- Patients live until around 16 years of age.
Duchenne's muscular dystrophy is an X-linked disease that affects...
- Predominantly affects boys
- Girls only
- Boys only
- Predominantly affects girls
Which of the following is the pathognomonic clinical feature of Duchenne's muscular dystrophy?
- Gower’s sign
- Milkmaid sign
- Darting motility
- Waddling gait
- Scoliosis
A 10-year-old boy presents with dyspnea and tachycardia. He has a history of progressive generalized weakness since the age of 3 years. His mother mentions that when he stands up, he uses his arms to push up his body. He also has slight calf muscle hypertrophy. Labs reveal elevated CK levels and the chest x-ray shows an enlarged cardiac shadow. Which of the following complication of the primary disease is most likely producing the symptoms?
- Dilated cardiomyopathy
- GBS
- Anemia of chronic diseases
- Scoliosis
- Obstructive sleep apnea
Author of lecture Muscular Dystrophy in Children

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture, easy to remember the difference between the two diseases. Our teachers should get a Lecturio subscription.
Clear explanation in a logical manner, luckily I found this few days before my final.
