Playlist
Show Playlist
Hide Playlist
Muscular Dystrophies

-
Slides Muscular Dystrophies.pdf.pdf
-
Download Lecture Overview
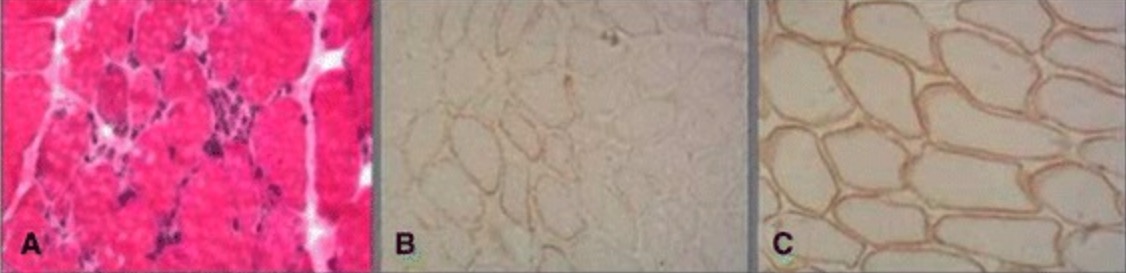
00:01 In this lecture, we're going to learn about the muscular dystrophies. 00:04 This is a really neat group of conditions. 00:07 And an important one to know about. 00:09 The muscular dystrophies are inherited muscle disorders. 00:12 So they differ from some of the acquired muscle pathology that we will talk about. 00:18 I think the best place to start when thinking about muscular dystrophies is how to organize them in your mind. 00:23 There are a lot of different muscular dystrophies that we'll go over, but a few that are common, were clinically relevant that we should know about, and some where you just need to know the names. 00:33 The first way to categorize muscular dystrophies is in their distribution of symptoms. 00:38 And this we'll see in the table here. 00:41 So we see there are some muscular dystrophies that present with proximal predominant weakness, there proximal disorders. 00:47 And the ones we think about are the X-linked muscular dystrophies: And that's Duchenne's Muscular Dystrophy, and Becker's Muscular Dystrophy. 00:55 Those are really important to understand. 00:57 They're the most common, and the most tested. 01:01 The second category of disorders, or distal predominant disorders. 01:05 They present with distal weakness. 01:07 And here we see myotonic dystrophy, which is abbreviated DM, not to be confused by Diabetes mellitus. 01:13 This is myotonic dystrophy, and some rare causes of Distal Muscular Dystrophy Welander's muscular dystrophy, the Dysferlinopathy's, and Hereditary inclusion body myositis. 01:26 The next two categories are more rare, but they're prominent in how they present. 01:31 Facial involvement in the muscular dystrophy should make us think of myotonic dystrophy type 1. 01:36 Fascioscapulohumeral Muscular Dystrophy, or FSHD, and Oculopharyngeal Muscular Dystrophy. 01:44 And then the last category is proximal and distal involvement. 01:48 So that combination of both proximal symptoms and distal symptoms. 01:52 And there we should think about Scapuloperoneal muscular dystrophy, Facioscapulohumeral muscular dystrophy, and myotonic dystrophy type 2. 02:01 So this categorization can really help us to break patient cases down, and clinical presentations down to a small list of muscular dystrophies. 02:09 We need to be concerned about. 02:12 So let's go back and talk a little bit about the pathophysiology of muscular dystrophies. 02:16 Why did these things happen? And what's going on at the level of the muscle to cause this symptom complex? Well, first of all, we remember that the muscle is made up of a sarcolemma, that's the cell membrane around the muscle. 02:29 External to that is the extracellular matrix. 02:32 And there's a protein complex that anchors the muscle to that extracellular matrix, and then to the muscle fibers. 02:39 And that protein complex is critical for allowing the muscle to move. 02:44 And dysfunction of that protein complex is going to lead to muscular dystrophies. 02:49 So what's the protein complex made of what's called the Dystrophin-associated protein complex. 02:54 And we'll learn about a number of enzymes that are involved in that. 02:58 And problems, mutations, with many proteins or any protein in that complex can give rise to a muscular dystrophy. 03:07 Laminin is an important protein that anchors the dystrophin-associated protein complex to the extracellular matrix. 03:14 And then dystrophin is a really important protein that we need to remember. 03:18 And that anchors the dystrophin-associated protein complex to actin. 03:23 And this is what really allows muscles to move. 03:26 It's that anchoring of the actin myosin to the extracellular matrix through the dystrophin- associated protein complex, and dystrophin itself. 03:36 In the muscular dystrophies, we see abnormalities in that complex. 03:40 There's an inability of the muscle to be anchored to the cytoskeleton and this results in two prominent histologic findings. 03:48 And these are important to remember. 03:50 So the first is myonecrosis. 03:52 Problems with that protein complex results in damage to the sarcolemma. 03:56 The immune system responds to that damage, and we see inflammation and damage necrosis of the muscle fibers. 04:03 And here we can see small purple cells. 04:06 There's the immune cells infiltrating into the muscle and resulting in inflammation and necrosis. 04:13 The second is we see muscle fiber loss or myofiber loss. 04:16 And this is characteristic of these conditions. 04:19 Patients present with weakness, and that's a result of myofiber loss. 04:23 Less pink muscle cell bodies, and more white fat and fibrosis. 04:28 And both of these findings are going to be important in how patients present. 04:32 Muscle necrosis is treated with prednisone and that's a common treatment that we utilize for these patients. 04:37 And the myofiber loss that we see and specifically with replacement of scar tissue can cause calf pseudohypertrophy, which will be a prominent clinical presentation and exam finding in these patients. 04:50 So, if we think back to that protein complex again laminin docking the dystrophin-associated protein complex to the sarcolemma anchored to dystrophin, and then to actin, and myosin. 05:01 What happens with the muscular dystrophy is to cause these histologic and clinical findings? Well, loss of dystrophin. 05:09 And that's the most common abnormality that we see in the muscular dystrophies particularly Duchenne's and Becker's Muscular Dystrophy results in the on anchoring of this protein complex to the sarcolemma. 05:21 We get breaks in the sarcolemma. 05:23 As you can see here, muscle enzymes are released into the systemic circulation. 05:28 The most common is CK. 05:29 And so we see elevated CK in these conditions. 05:33 And as a result of this damage, there's an immune infiltrate. 05:36 And I'll ultimately fibroblasts infiltration and scarring of the muscle that occurs. 05:44 So the prototypical findings that we see in the pathophysiology is inflammation followed by fibrosis and loss of muscle fibers. 05:51 The muscle is replaced by fat and fibrosis. 05:54 The CK is elevated and significantly elevated. 05:57 More than 10,000 times the upper limit of normal. 06:00 And that degree of elevation really should point us towards a muscular dystrophy. 06:05 And the pathophysiology is dystrophic changes within the muscle and that's that myonecrosis and myofiber loss. 06:12 Clinically, we see that this leads to weakness. 06:14 Often, proximal weakness but any distribution we can see. 06:18 And then pseudohypertrophy as a result of the fibrosis in muscles.
About the Lecture
The lecture Muscular Dystrophies by Roy Strowd, MD is from the course Hereditary Neuromuscular Disorders.
Included Quiz Questions
Which of the following disorders is characterized primarily by facial muscle involvement?
- Oculopharyngeal muscular dystrophy
- Duchenne’s muscular dystrophy
- Myotonic dystrophy type 2
- Becker’s muscular dystrophy
- Welander’s muscular dystrophy
A muscle sample is sent to pathology for analysis. Which of the following characteristics would indicate a possible muscular dystrophy?
- Myonecrosis
- Nuclear clearing
- Spindle-fiber formation
- Type I fibers
- Type II fibers
Duchenne’s muscular dystrophy is caused by a mutation in which of the following components of the sarcomere?
- Dystrophin
- Actin
- Laminin
- Sarcolemma
- Extracellular matrix
Author of lecture Muscular Dystrophies

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
