Playlist
Show Playlist
Hide Playlist
Radial Nerve Injury

-
Slides 05 Mononeuropathy Neuropathology II.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
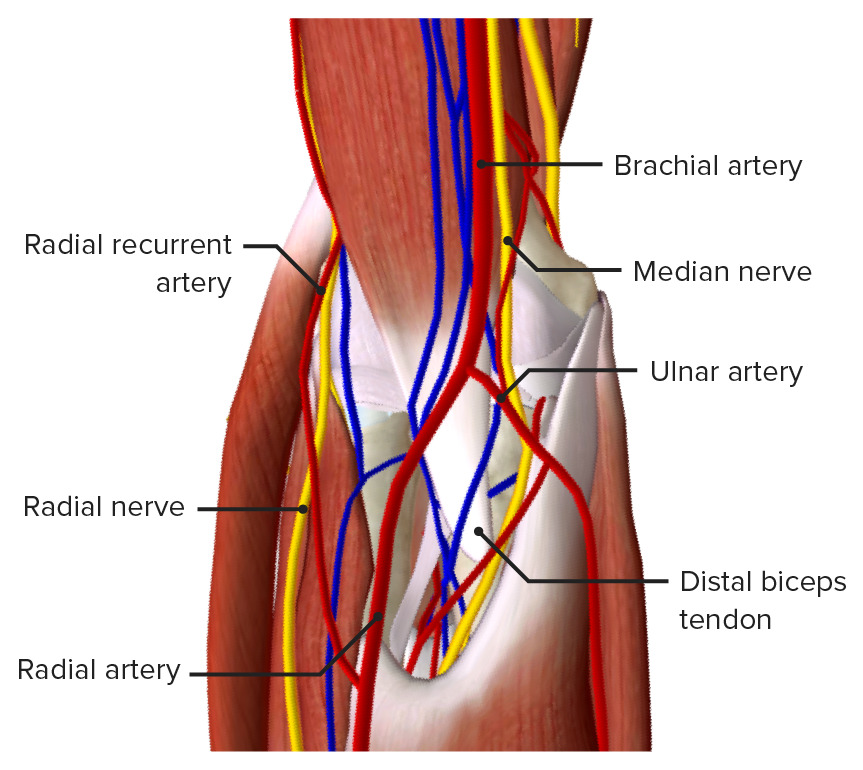
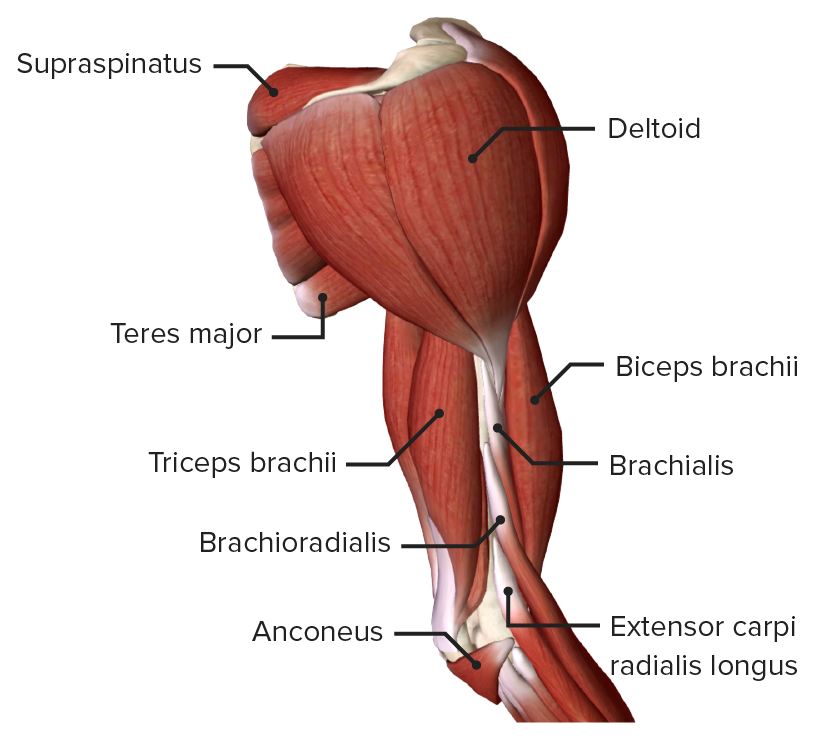
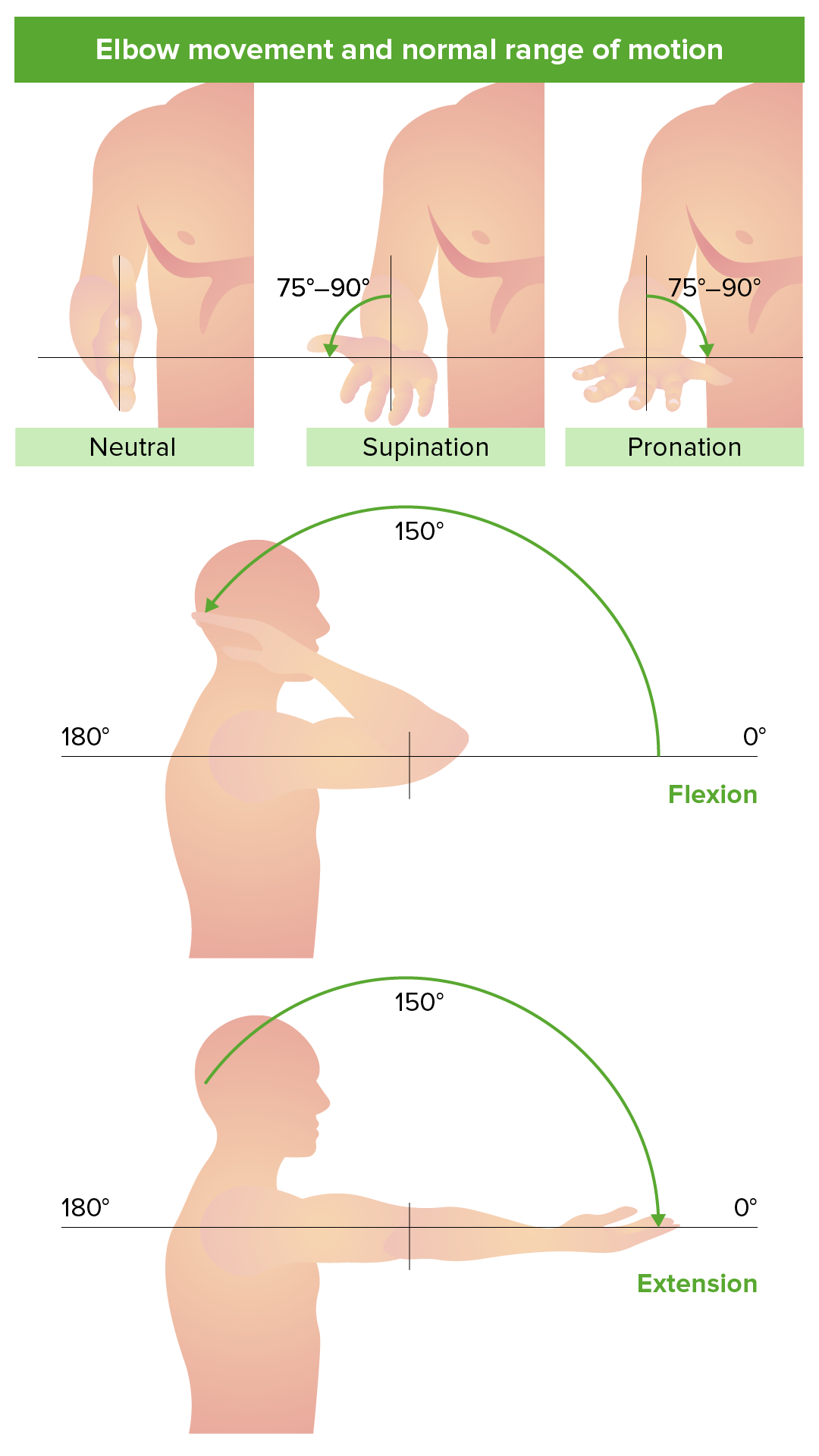
00:01 Here, we’ll take a look at continuation of peripheral neuropathy. 00:05 We looked at plexopathies and we looked at the roots in greater detail including Erb’s and Klumpke. 00:11 Here, we’ll take a look at individual nerves that has been damaged, mononeuropathy. 00:16 And which particular nerve has been damaged is important. 00:19 So here, commonly, a site of injury will be the radial nerve. 00:23 Most commonly at the spiral groove of the humerus. 00:27 That’s extremely important anatomically. 00:30 How did it occur? It could be at the side of the axilla. 00:33 Now, think about where you are. 00:35 And I know that many of you have heard of Saturday night palsy, but what does that actually mean? Well, during the evening, shall we say you’re at a club or a bar or whatever and as you continue to indulge, and then at some point in time, maybe you’re sitting on a stool. 00:51 And on a stool, you put your arm back on your arm chair, and you are not in your proper senses, and you have forgotten that you left your arm there over the arm chair and therefore causing compression of the axilla. 01:07 That’s really what this is about. 01:09 Practically speaking, look at crutches. 01:12 Where do you place crutches? On the axilla. 01:14 And so therefore may cause injury to the radial nerve. 01:20 If you take a look at the schematic here, I want you to focus upon the radial nerve that you see. 01:25 And so therefore, in the forearm, the posterior interosseous syndrome is something that you want to keep in mind as well for the radial nerve, please. 01:35 Clinical features include wrist drop, patient unable to extend wrist or fingers up. 01:42 Wrist drop. 01:43 Flexion. 01:45 Occasional forearm, maybe hand and thumb numbness could also be seen as well with radial nerve damage. 01:53 Risk factors: Diabetes, alcoholism, leaning on arms or axilla, sleeping in the wrong position perhaps. 02:02 Trauma. 02:03 Lead poisoning, of course, may cause issues with demyelination or mononeuropathy in many of the nerves, but here, specifically, a possible risk factor. 02:17 Physical examination: Wrist drop with inability to extend your fingers as we talked about. 02:22 And then check the three following muscles: Triceps: ask the subject to extend the elbow. 02:32 Brachioradialis: ask the subject with thumb pointing to ceiling to flex the forearm. 02:45 Extensor indicis proprius: with the hand flat on a bed, ask subject to raise index finger up. 02:59 Occasional numbness/decreased sensation over dorsum of the hand or thumb may be seen. 03:04 Dorsum. 03:07 Difficulty spreading the fingers, pseudo-ulnar interossei weakness. 03:13 Correctible when wrist is held with level with forearm by examiner. 03:19 These are important physical exams for radial nerve. 03:23 They're fairly localized. 03:25 So three possible locations determined by exam, triceps, brachioradialis, and extensor indicis proprius. 03:35 Axilla: Triceps, brachioradialis, extensor indicis proprius, all weak. 03:44 If it’s the humeral spiral groove, triceps strength is normal. 03:51 Weak brachioradialis and weak extensor indicis proprius. 03:55 Forearm, posterior interosseous syndrome: triceps and brachioradialis are normal. 04:01 But then the extensor indicis proprius is weak. 04:06 Spend a little bit of time with proper physical examination with that of the radial nerve because it is a common site of injury and the three possible locations that we’ve walked you through in greater detail. 04:21 Differential diagnosis: If the other nerves are involved, it could be a brachial plexus lesion Don’t make a mistake of diagnosing a superimposed ulnar neuropathy because the interossei “appear” being weak. 04:36 Remember the pseudo that we talked about earlier. 04:41 Bilateral radial palsies. 04:43 Always look for lead poisoning. 04:45 Remember, lead poisoning is not just restricted to one nerve. 04:48 So you want to think of it as being a differential. 04:51 And so therefore, if there’s bilateral, then maybe your lead is the culprit. 04:56 Very rarely, very rarely, but nonetheless. 05:00 We’ll talk about myotonic dystrophy in greater detail. 05:02 It could cause weakness, but you also have wasted forearm and bilateral wrist drop. 05:08 Once again, with myotonic dystrophy as being a differential diagnosis. 05:13 Usually, it’s not going to just be one. 05:17 Recommendations: Wrist/fingers splint to keep the fingers extended in moderate to severe axonal lesions. 05:26 Passive wrist/fingers range of motion to maintain mobility. 05:31 That actually becomes of utmost importance. 05:34 The longer that a particular position is held, there’s every possibility that further damage could be caused and that’s extremely important. 05:40 You want to make sure that mobility is always somehow maintained.
About the Lecture
The lecture Radial Nerve Injury by Carlo Raj, MD is from the course Mononeuropathy.
Included Quiz Questions
Which of the following examinations is NOT an assessment of the function of the radial nerve?
- Shoulder extension
- Thumb abduction at the wrist
- Extension of the four medial digits of the hands
- Wrist extension
- Extension of the forearm
A patient presents with a weak brachioradialis, a weak extensor indicis proprius, and normal triceps strength. Where is the possible injury to the lesion?
- Humeral spiral groove
- Axilla
- Medial epicondyle
- Wrist
- Spinal roots
Which of the following etiologies is the most likely cause of bilateral wrist drop?
- Lead poisoning
- Amyotrophic lateral sclerosis
- Spiral fracture of humerus
- Hypercalcemia
- Nerve root injury
Author of lecture Radial Nerve Injury

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
