Playlist
Show Playlist
Hide Playlist
Metanephrines

-
Slides PheochromocytomaMENSyndrome Surgery.pdf
-
Download Lecture Overview
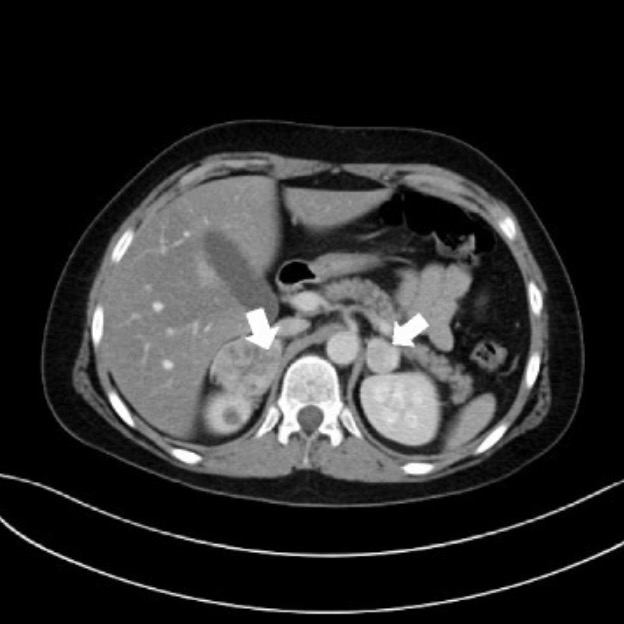
00:01 Let me ask you a question. What are metanephrines since they are so important to the diagnosis of pheochromocytoma? I’ll give you a second to think about this. That’s right. Metanephrines are catecholamine metabolites. Let’s take a look at how this works. As a reminder, catecholamines include substances called norepinephrine or epinephrine. These medications or substrates may actually be familiar to you in the sepsis lectures. Norepinephrine and epinephrine undergoes series of oxidative reactions by a very, very important enzyme called monoamine oxidase. 00:42 Do you recall where monoamine oxidase may be pertinent in other series? Norepinephrine and epinephrine subsequently turn into their metabolite after these oxidative reactions into normetapinephrines or metanephrines. This is what we measure in the urine or the plasma. 01:02 Remember, monoamine oxidases are very important and MAO inhibitors in your psychiatry lectures. 01:11 Now, let’s move on to diagnostic imaging. Endocrine societies of America recommend the first line imaging as a cross-sectional CT scan of the abdomen/pelvis. Remember, importantly for the vast majority of detection of tumors by CT scan, it’s only sensitive for lesions greater than 1 cm. 01:30 You’ll notice by the green arrow pointing at an organ just above the kidney on the left side, this is an adrenal gland. Typically speaking, the adrenal gland is a small organ. 01:42 This is about three times the normal size. In pregnant women or patients where it’s difficult to identify based on CT scan of the abdomen/pelvis, MRI can be a very important modality. 01:57 In this image, take a look at the white arrow. The white arrow once again points to the similar left adrenal gland above the kidney. Above the MRI image is a surgical specimen of the removed adrenal gland. Now, let’s think upon a scenario where the CT scan and the MRI cannot localize where the adrenal gland is or where the pheochromocytoma is. I like to introduce you to an MIBG scan. This is a radioactive scan using radiotracer iodine-123 scintigraphy. MIG is a substrate for norepinephrine transport. Therefore, any hyperactivity of the transporter such as a pheochromocytoma would light up as a hot spot on this MIBG scan. Now, if you’re presented with a clinical scenario and the question is what is the next diagnostic image study of choice? Remember, don’t pick the MIBG scan first because we recommend use of MIBG scan only if the CT and MRI cannot locate the lesion.
About the Lecture
The lecture Metanephrines by Kevin Pei, MD is from the course General Surgery.
Included Quiz Questions
A patient with chronic, refractory hypertension presents with severe headaches, episodic sweating, and palpitations. Urine catecholamines and metanephrines are elevated. What is the first-line imaging study used to locate the suspected pheochromocytoma?
- Computed tomography of the abdomen and pelvis
- MRI
- Plain abdominal x-ray
- MIBG scan
- Abdominal ultrasound
What is the mechanism of the MIBG scan?
- Radioactive uptake of the substrate for the norepinephrine transporter
- Radioactive uptake of oxidative catecholamine metabolites
- Radioactive uptake of monoamine oxidase
- Radioactive uptake of norepinephrine and epinephrine in the adrenal medulla
- Radioactive uptake of metanephrine in the adrenal medulla
What is the minimum size of a tumor in the adrenal gland which can be detected on CT scan?
- 1 cm
- 1 mm
- 0.5 cm
- 2 cm
- 5 cm
Author of lecture Metanephrines

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
