Playlist
Show Playlist
Hide Playlist
Mesothelioma



-
Slides PulmonaryNeoplasia RespiratoryPathology.pdf
-
Download Lecture Overview
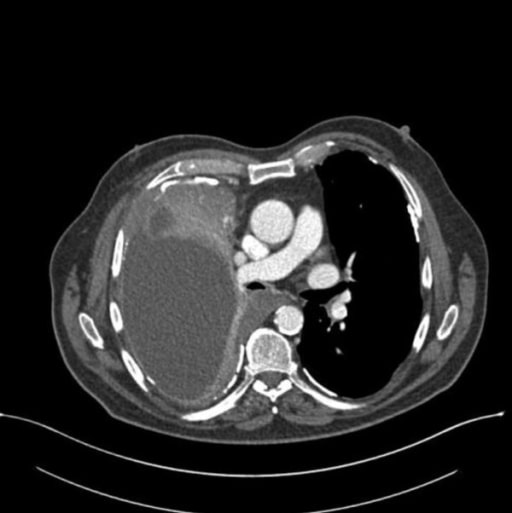
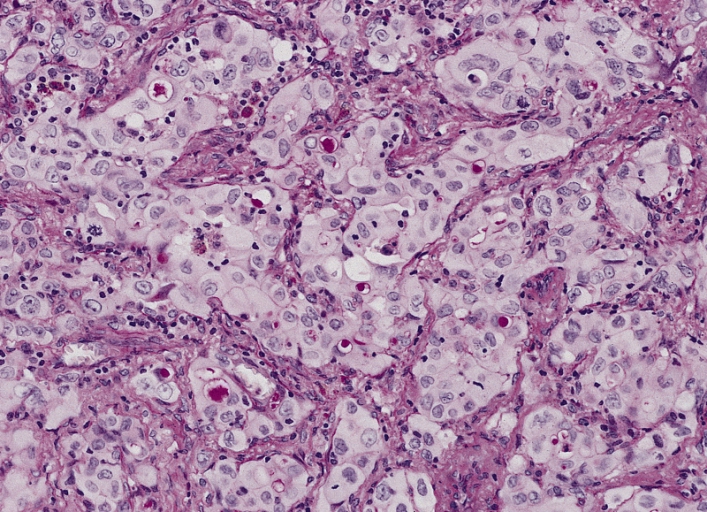
00:00 Now, let's move on. 00:02 Mesothelioma is where we are. 00:03 Mesothelioma, remember, the only real precursor, the only precursor that can give rise to mesothelioma is asbestos. 00:12 With asbestos, who’s your patient? Maybe a roofer, maybe a plumber, maybe there was non-environmental, maybe you’re washing the clothes of an individual that was dealing with asbestos. 00:23 Right? Now, what happen next? There are two different type of fibres. 00:28 One was the amphibole. 00:30 That was a crocidolite. 00:32 And the other one was the serpentine and that was the chrysotile. 00:36 The one that was dangerous was the amphibole. 00:38 Okay. 00:39 This may then give rise to mesothelioma. 00:42 This is a malignancy of the pleura associated with asbestosis. 00:49 Smoking is not the factor. 00:51 Clear? So, now, we have two major lung cancers where smoking is not a factor. 00:57 We have adenocarcinoma in bronchogenic and then mesothelioma, but this is dealing with asbestos, may result in haemorrhagic pleural exudative effusion. 01:09 Thickened pleura. 01:11 Let's take a look at the histology of mesothelioma. 01:14 They might describe the psammoma bodies as being calcium deposit. 01:17 Is that clear? That is a psammoma body and that of course is completely non-specific. 01:22 You can find that in many cancers, including meningioma. 01:25 You can find this in, what’s the most common thyroid cancer? Papillary cancer of the thyroid. 01:31 So, you can find this in many. 01:32 Here in mesothelioma as well. 01:34 Cytokeratin and what’s some of this? Calretinin. 01:38 Positive in almost all mesotheliomas whereas calretinin is almost always negative in most carcinomas. 01:50 So that’s extremely specific, when it comes to mesothelioma, one thing that I wish to bring to your attention is when you have asbestosis, an asbestos. 01:58 What was that pathognomonic lesion that we found in the lung? Oh yes, that was pleural plaque and I told you at that time because there might be pleural plaque, that it’s not a precursor to mesothelioma. 02:09 I wish to repeat that very statement once again. 02:12 You are involving the pleura here in mesothelioma, no doubt. 02:15 It’s a malignancy. 02:16 You can expect it to be bloodiness, unfortunately. 02:21 Lung cancer is the leading cause of mortality from cancer. 02:24 Presentation, cough, haemoptysis, bronchial constriction, wheezing. 02:31 The pneumonic "coin" lesion on chest X-ray or non-calcified nodule on CT. 02:38 So, “coin” lesion on X-ray. 02:40 Literally looks like one nodule. 02:42 Non-calcified nodule on CT. 02:45 The sites of metastasis from the lung include adrenal, brain, bone, liver. 02:56 Metastasis to the lung from the breast, colon, prostate, bladder cancer. 03:05 Liver can be put in there as well. 03:07 So, it’s from the lung to these organs, from these organs to the lung. 03:14 Breast being a big one. 03:17 Complications. 03:19 What may then happen if you have a lung cancer in which, well, on the right side, it causes compression of the superior vena cava? It’s called superior vena cava syndrome. 03:30 Therefore what happens? Flushing of the face because you can’t drain your upper extremities. 03:36 Is that clear? Do not confuse this with superior sulcus syndrome. 03:42 Here, the patient is not going to have flushing of the upper face and upper extremity. 03:47 It’s a fact that this patient has drooping of the eyelid. 03:51 There’s going to be the pupils that are rather tiny and there’s absolutely no sweating. 03:58 What happened? Well, this was a tumour, maybe a small cell lung cancer in the apex of the lung. 04:05 Understand, Pancoast, as you here, is not a separate lung cancer. 04:11 Do you understand that? It is a existing lung cancer that happens to be superior sulcus causing compression of the... 04:21 Good, sympathetic chain. 04:23 So therefore you have unrestricted, unregulated parasympathetic activity on the pupil. 04:30 Pimple pupil miosis. 04:33 You’re going to have absolutely no sympathetic activity on your sweat glands. 04:37 Therefore, you’re going to have anhydrosis. 04:40 And number 3, the droopy eyelid, ptosis. 04:43 Welcome to Horner. 04:45 Do not forget the other name, known as superior sulcus. 04:48 I beg you not to get this confused with superior vena cava syndrome, where the patient will have flushing in the head and such. 04:56 Paraneoplastic syndromes, we’ve talked about plenty. 04:58 You tell me about ADH and ACTH. 05:00 Small cell. 05:01 If it’s PTHrP, it will be squamous cell. 05:05 Hoarseness, how is this occurring? “Doc, I’m having a hard time.” Well, this is going to be recurrent laryngeal nerve. 05:11 And as far as the effusions are concerned, these will be haemorrhagic or bloody, either pericardial or pleural.
About the Lecture
The lecture Mesothelioma by Carlo Raj, MD is from the course Lung Cancer .
Included Quiz Questions
Which of the following complications may arise from superior sulcus syndrome?
- Horner syndrome
- SIADH
- Flushing of the face
- Hypercalcemia
- Pleural effusions
What pneumoconiosis is associated with the development of mesothelioma?
- Asbestosis
- Berylliosis
- Coalworker’s pneumoconiosis
- Byssinosis
- Silicosis
Which of the following is NOT associated with the development of mesotheliomas?
- Pleural plaques
- Pleural exudative effusion
- Calretinin
- Cytokeratin
- Psammoma bodies
Author of lecture Mesothelioma

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I generally love the way he teaches, It's very clear and he makes you think in the process.
