Playlist
Show Playlist
Hide Playlist
Melanoma


-
Slides Melanoma Surgery.pdf
-
Download Lecture Overview
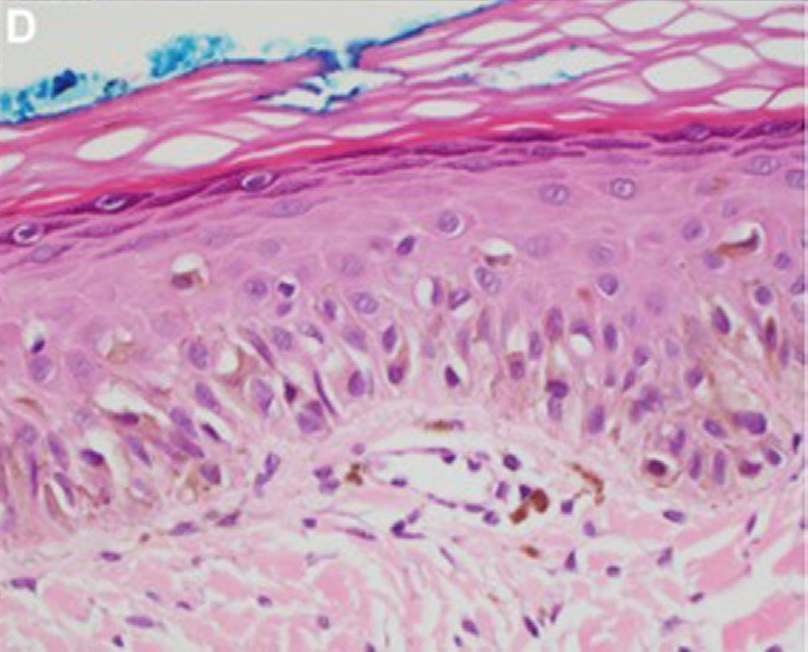
00:01 Thanks for joining me on this discussion of melanoma. 00:07 Melanoma is a malignancy of melanocytes which produces our pigments. 00:12 This is variable expression of the melanocytes and the pigmentation is the reason why we all have different skin colors. 00:21 Here, in this image, you notice the different versions of melanoma on various parts of the body. 00:27 The risk factors for melanoma include sun exposure, family history of melanoma or skin cancers, a personal history melanoma or skin cancers, and dysplastic nevus. 00:40 This is why it’s important to elicit a thorough history. 00:43 This is particularly true about sun exposure and multiple sunburns. 00:48 That's why melanoma is more likely in fair skinned patients. 00:53 The different subtypes of melanoma depend on morphology and severity. 00:59 The first and most common type is the superficial spreading melanoma, which is usually associated with previously present nevus. 01:05 The second type is lentigo maligna, commonly in sunburnt areas. 01:09 Acral lentignous melanoma which arise most commonly on palmar, plantar, subungual and occasionally mucosal surfaces is the third type. 01:18 It is common in dark-skinned individuals. 01:20 And the last subtype is nodular melanoma which are vertical growth phase melanomas. 01:24 On physical examination, it's very important to completely disrobe the patient and not only look at the front but also the back. 01:30 Remember, much of the sun exposure, particularly on beaches is actually on the back. 01:35 This is a difficult area for the patient to examine themselves. 01:38 So as clinician, you have to do a thorough examination. 01:41 There are some very important physical findings when characterizing melanoma. 01:44 For every patient in every melanoma potential lesions, we want to look at ABCDE system. 01:50 A for asymmetry, B, take a look at the lesion, does it have jagged irregular borders, that's more concerning. 01:56 Next C, take a look at the color, pigmentation itself is associated with a likelihood of a cancer. 02:03 Then D, diameter, if the lesion have a size greater than 6 mm, they may have more of a chance of harboring cancer. 02:09 And lastly, the E is for evolution or a change in size and color. 02:13 Unfortunately, no lab - routine laboratory values are likely to be helpful. 02:22 Sometimes, an LDH value is gotten to follow the patient after surgical cure. 02:28 When you’ve made the diagnosis of melanoma, it's important to make sure that the patient has not had a metastasis. 02:35 It’s important to do a metastatic workup with a CAT scan cross-sectional imaging of the chest, abdomen and pelvis. 02:43 Unfortunately, in this patient, you see many, many liver metastases. 02:48 Sometimes, preoperatively, patients undergo a CT PET scan. 02:53 In general, oncologic processes are PET-avid, meaning glucose that has tagged nuclear medicine is likely to be up-taken at a higher rate in cancers than normal tissue. 03:07 In this unfortunate patient with metastatic melanoma, you see multiple regions in the chest and the abdomen that is hot on a PET scan. 03:16 Now that you've decided the patient is appropriate for surgery, what margins do you need for this oncologic process? For melanomas, the depth of invasion based on your biopsy is the single most determinant of the necessary margins. 03:31 For example, in thin melanomas, or 1 mm or less, we usually require 1 cm disease-free margin. 03:39 Between 2 and 4 mm, we require 2-cm margin. 03:45 And those that are greater than 4 mm, we’re not exactly sure how much more of a margin we need, but they definitely need to be at least 2 cm. 03:54 Remember, much like the breast lectures, sometimes patients with melanoma have lymph node metastases. 04:01 These lymph node metastases have poor prognosis. 04:05 And much like breast diseases, sometimes patients undergo sentinel lymph node biopsies. 04:10 Sentinel lymph node biopsies of melanoma is by the same theory that, generally speaking, one or two nodes is the sentinel node of the draining basin. 04:20 It is worth mentioning that adjuvant immunotherapy with interferon or ipilimumab has an emerging role following staging in appropriately selected patients. 04:29 Now, it's time to revisit some clinical pearls and high-yield information. 04:35 Remember, melanoma has multiple variants histologically, but the workup is the same, including the metastatic workup. 04:42 Generally, the treatment is the same as well in terms of surgery. 04:46 And also remember, melanoma is one of the most common sources of small bowel metastases. 04:52 Remember, metastases to the small bowel, think melanoma on your clinical examinations. 04:58 Thank you very much for joining me on this discussion of melanoma.
About the Lecture
The lecture Melanoma by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
What is the size of excision disease-free margin required for melanoma with 1 mm depth?
- 10 mm
- 2 mm
- 3.5 mm
- 15 mm
- 20 mm
A melanoma with depth >4 mm requires at a minimum what margin for excision?
- > 2 cm
- 1-4 cm
- 4 cm
- > 4 cm
- 1 cm
Author of lecture Melanoma

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
It is useful for anybody who wants to learn accurately and perfectly. All aspects are clearly pfesented
