Playlist
Show Playlist
Hide Playlist
Male Hypogonadism with Case

-
Slides Reproductive Endocrine Disorders.pdf
-
Reference List Endocrinology.pdf
-
Reference List Reproductive Endocrine Disorders.pdf
-
Download Lecture Overview
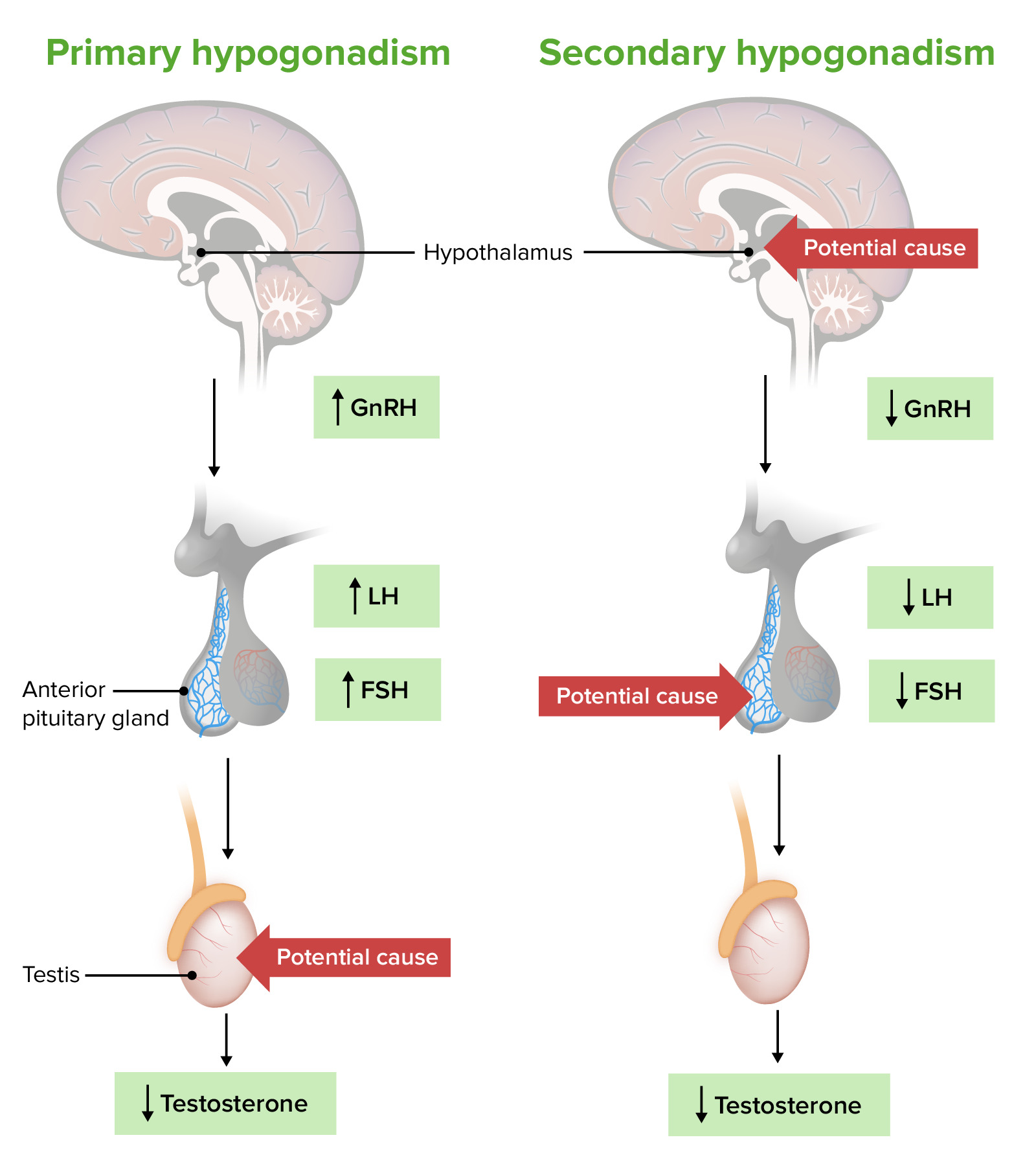
00:01 Let's go on to male hypogonadism. 00:04 This clinical syndrome results from failure of the testes to produce physiologic levels of testosterone and normal numbers of sperm due to disruption of the hypothalamc and pituitary testicular axis. 00:15 It can be primary, in the case of testicular abnormalities or secondary in the case of pituitary dysfunction where GnRH and FSH and LH are deficient. 00:29 Causes of hypogonadism are numerous and are divided into primary and secondary. 00:34 Primary would primarily affect the testicles and secondary would be another cause, usually of the endocrine axis. 00:43 Dealing with the primary cause is infection such as mumps which is a viral infection with orchitis which is inflammation of the testicles, is a significant cause of hypogonadism. 00:54 It can also be a consequence of radiation treatments for conditions like testicular malignancies or lymphomas. 01:01 It can also occur when taking chemotherapy agents or other toxins. 01:05 When there is being testicular trauma or testicular torsion, and then in Klinefelter syndrome which is 47,XXY tends to be the most common congenital cause. 01:17 Under these situations, you would look for the following clinical characteristics: Very tall stature, small testes, developmental delay and patients manifesting socialization and other psychological abnormalities. 01:32 Moving on to secondary hypogonadism. 01:35 Kallman syndrome, which is associated with anosmia is a pituitary cause. 01:41 Also, hyperprolactinemia, medications that affect secretion of GnRH or FSH and LH Critical illness, untreated sleep disorders which usually manifest as central sleep apnea, Obesity which can also contribute not only to the condition a priori but also through sleep disorders and central sleep apnea. 02:05 Liver and kidney diseases, alcohol and marijuana use, eating disorders and finally, trauma, this time to the head as opposed to the testicles. 02:14 Let's go on to a case that overviews a 45 year old man, who is evaluated for the management of tiredness and reduced libido, a very common presentation in general medical practice. 02:27 Medical history is significant for hypertension and hyperlipidemia. 02:32 Medications are hydrochlorothiazide and atorvastatin. 02:36 On physical exam, his vital signs are normal. 02:39 He has normal hair distribution, no gynecomastia and an unremarkable testicular exam. 02:45 Lab studies obtained at 6 PM revealed a total testosterone level of 210 ng/dL and an LH level of 5 mU/mL What should one do next? So, going through this case, the low libido and fatigue suggest that the patient has a low testosterone level. 03:06 A testosterone level should be checked at 8 AM, the diagnosis is then confirmed if he has two separate measurements at 8 AM that are both low. 03:17 This particular patient did indeed have a low testosterone level and a low luteinizing hormone level at 5 mU/mL In the setting of low libido implying that he has secondary hypogonadism. 03:31 Measuring at 8 AM testosterone level is indicated in men with symptoms of hypogonadism. 03:36 If the testosterone level is low, a second level is then checked the following day, again at 8 AM. 03:43 The diagnosis is made with a low serum testosterone measurements. 03:48 Measurements of free testosterone is appropriate in obese men because obesity will lower the sex hormone binding globulin and will lead to falsy low measured total testosterone levels. 03:58 If the testosterone is low, a serum luteinizing hormone is then measured. 04:03 If this is elevated, primary hypogonadism is the diagnosis. 04:07 If the luteinizing hormone level is low, then it would suggest secondary hypogonadism. 04:13 Further evaluations of these patients is usually directed to identifying the cause of the elevation or decrease in luteinizing hormone. 04:24 Treating hypogonadism is usually in the form of a testosterone therapy which can be initiated after the etiology has been determined. 04:33 The goal is to replace testosterone so that the measured total testosterone value is in the mid to normal range. 04:40 Testosterone replacement should be in the form of a gel, a patch or an injection to avoid the phenomenon whereby testosterone that's taken orally is heavily metabolized by the liver during first pass. 04:52 Testosterone therapy have clinical benefits that include an increase in libido, an increase in lean muscle mass and fat free mass and also in bone density and improvement in secondary sexual characteristics. 05:06 Potential adverse effects include acne, their impact to the prostate, so they should be avoided in patients who have a history of prostatic carcinoma, also in patients who have a history of obstructive sleep apnea and then hematologic effects are significant. 05:20 Patients tend to develop an increase in their red cell volume, otherwise known as erythrocytosis and they can also have an increase in their platelets or thrombophillia. 05:29 The thrombophillia can lead to the occurrence of blood clots and the thrombocytosis may contribute to sluggish circulation. 05:37 Patients should be counseled on the decreased fertility that's associated with exogenous testosterone therapy. 05:44 Testosterone therapy is only indicated for the treatment of testosterone defficiency. 05:49 It is not used for impaired spermatogenesis. 05:52 So if the patient desires fertility, it is a good idea for them to know this prior to taking testosterone replacement.
About the Lecture
The lecture Male Hypogonadism with Case by Michael Lazarus, MD is from the course Reproductive Endocrine Disorders. It contains the following chapters:
- Male Hypogonadism
- Case: 45-year-old Man with Tiredness and Decreased Libido
- Hypogonadism – Diagnosis
Included Quiz Questions
Which of the following viral infections is most likely to cause inflammation of the testes, leading to primary hypogonadism?
- Mumps
- Measles
- Chickenpox
- Smallpox
- Rubella
Which is the most common congenital cause of primary hypogonadism in male patients?
- Klinefelter syndrome
- Turner syndrome
- Down syndrome
- Marfan syndrome
- Fragile X syndrome
Which investigation most likely confirms the diagnosis of hypogonadism in male patients?
- Decreased 8 AM testosterone levels
- Increased 8 AM testosterone levels
- Decreased 8 AM estrogen levels
- Increased 8 AM estrogen levels
- Decreased 8 PM progesterone levels
Which of the following is NOT an adverse effect of testosterone therapy?
- Anemia
- Acne
- Thrombophilia
- Prostate hyperplasia
- Obstructive sleep apnea
Author of lecture Male Hypogonadism with Case

Michael Lazarus, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
