Playlist
Show Playlist
Hide Playlist
Labor Stage 1: Normal and Abnormal Labor

-
Slides LaborStage1 Obstetrics.pdf
-
Download Lecture Overview
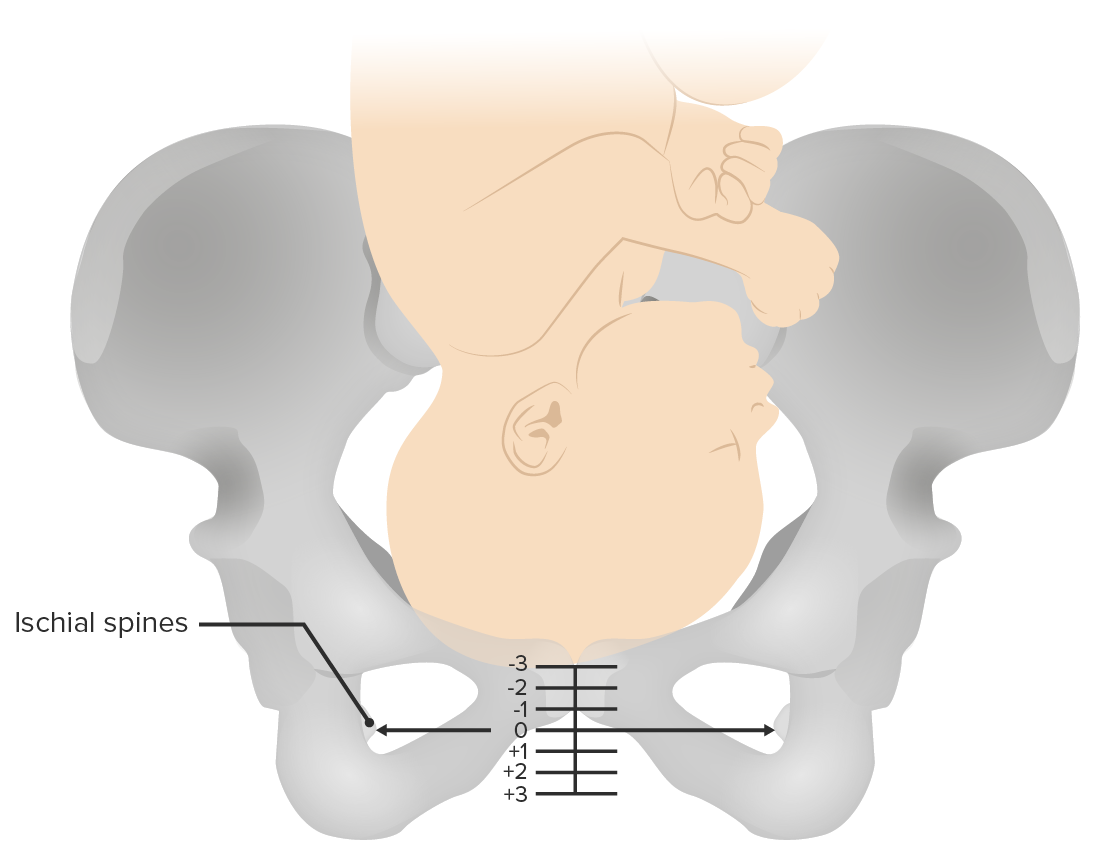
00:01 Now let's discuss the first stage of labor. 00:05 So in review of all of our stages of labor, let's remember that Stage 1 starts from onset of labor until 10 centimeters dilated. 00:13 Stage 2 is 10 centimeters dilated until the delivery of the infant. 00:17 And Stage 3 starts with the delivery of the infant and ends with delivery of the placenta. 00:22 So in Stage 1 we have contractions that are causing cervical change and they are also causing the fetus to descend in the pelvis. 00:30 We can further divide Stage 1 labor into the latent phase, which is the onset of contractions that continue until the cervix is about 4 to 6 centimeters dilated, and the active phase, which is from 6 centimeters dilated to 10 centimeters dilated. 00:45 Now, we have some parameters that we considered to be normal for the first stage of labor. 00:51 For primiparous, well, I mean in latent labor, we expect that to last under 20 hours, for a multiparous, we expected it to last under 14 hours. 01:01 In the active phase we expect the cervix to change 1.2 centimeters per hour for out first time moms. 01:07 And 1.5 centimeters per hour for our multiparous moms. 01:11 So we have an abnormal first stage labor. 01:16 What causes that? Well, when we think of the 3 P's. 01:18 Power, Passenger and Pelvis. 01:22 With power we're talking about the strength of contractions. 01:27 Now how do we measure the strength of the contractions. 01:30 Typically in labor our moms are going to have a monitor on that tells us them externally how often they are contracting. 01:36 If we want to know how strong the contractions are, we place an intrauterine pressure catheter that measures something called "The Montevideo Units." The Montevideo units are a measurement that are taken over 10 minute strip looking at all of the contractions and measuring the area under the curb. 01:56 We expect it to be 180 to 220 Montevideo units to say the contractions are adequate. 02:02 If those contractions are not adequate, we're going to start a medication called Pitocin. 02:08 This is a synthetic form of oxytocin and this makes the contractions stronger. 02:12 Now our next P is passenger. 02:17 So what can go wrong with our passenger to make the first stage of labor abnormal. 02:22 Well we could have malrepresentation of our passenger such as a breech presentation, a face presentation or brow presentation. 02:28 That will prevent the passenger from coming down the pelvis. 02:31 Or the passenger could be having fetal heart rate issues. 02:35 Now, our next P is the pelvis. 02:38 Now there is no way to determine what type of pelvis a patient has prior to labor. 02:45 But just to note, there are 4 different types of pelvises. 02:49 And depending on the type of pelvis that can ease the delivery or it can make the delivery more difficult. 02:55 So the gynecoid pelvis is one that allows the head to always rotate to also put anterior making vaginal delivery pretty easy. 03:04 Anthropoid pelvis more common in African American women cause the fetal head to rotate to the occipit posterior position. 03:13 While they can still have a vaginal delivery, sometimes that can be a little difficult. 03:17 And sometimes it requires an operative vaginal delivery to get those last little maneuvers to have the fetal head go underneath the pubic symphysis. 03:24 The platypeloid pelvis will cause the fetal head to be in a transverse position. 03:30 If you remember from our previous lecture, we need that fetal head to occipit anterior or occipit posterior so that only 9 and half centimeters of the fetal vertex is trying to pass through the pelvis. 03:41 Remember that the fetal pelvis is largest at 10 centimeters at it's largest point. 03:46 A transverse presentation is not going to be able to be pass through the pelvis. 03:51 And an android pelvis is more like a guy's pelvis and that is heart shaped. 03:57 And in this type of presentation the fetal head has difficulty even engaging.
About the Lecture
The lecture Labor Stage 1: Normal and Abnormal Labor by Veronica Gillispie, MD, MAS, FACOG is from the course Intrapartum Care. It contains the following chapters:
- First Stage of Labor
- Stage 1 – Normal Labor
- Stage 1 – Abnormal Labor
Included Quiz Questions
A G1PO woman at 41 weeks gestational age is experiencing about 5 contractions every 10 minutes, and her cervix has dilated from 5 cm to 6 cm over the past 3 hours. On cervical exam, fetal sutures are felt and confirmed to be in the occiput anterior position at -1 station. What is the next step in management?
- If external intrauterine pressure measurement is insufficient, an intrauterine catheter should be placed.
- She should be started on Pitocin to increase the frequency of her contractions.
- She should be given a cervical ripening agent to soften the cervix.
- She should be managed expectantly for spontaneous vaginal delivery with no further intervention.
- She should go for a cesarean section.
A G2P1 woman at 38 weeks gestational age with a past history of normal vaginal delivery is on the ward in active labor. Her cervical exam has remained unchanged at 6 cm dilation, 60 % effacement, and -3 station. She is feeling painful contractions every 2-3 minutes and an intrauterine pressure catheter measures the power of her contractions as 200 Montevideo units. What is the next step in management?
- Evaluate for fetal malpresentation
- Start Pitocin to increase the strength of her contractions
- Start Pitocin to increase the frequency of her contractions
- Vacuum-assisted delivery to help the baby descend into the pelvis
- Administer a cervical ripening agent to soften the cervix
What pelvic shape allows for easiest delivery?
- Gynecoid pelvis
- Anthropoid pelvis
- Platypelloid pelvis
- Android pelvis
- Cuboid pelvis
Into which position does the gynecoid pelvis rotate a fetus?
- Anterior occiput
- Posterior occiput
- Transverse anterior
- Transverse posterior
- Right anterior transverse
Author of lecture Labor Stage 1: Normal and Abnormal Labor

Veronica Gillispie, MD, MAS, FACOG
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
well explained and detailed content and structure for easy understanding and memorization
I Really liked it. The example you gave with the wedding was perfect, I will never forget it.
