Playlist
Show Playlist
Hide Playlist
Innervation of the Ocular Muscles – Anatomy Review

-
Slides Structures of the eye.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
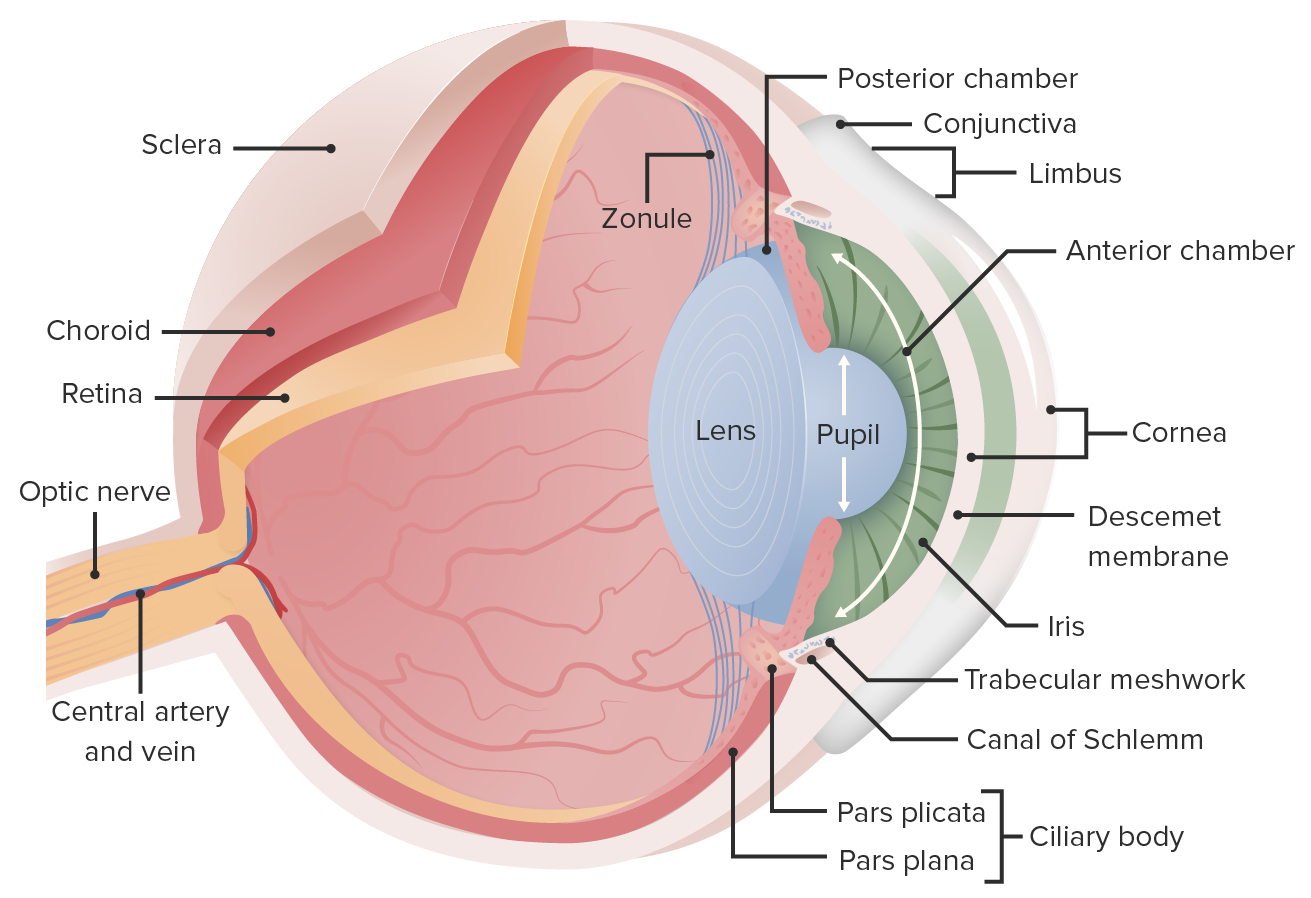
00:02 Welcome back, we're going to talk more about some of the important, larger structures of the eye. 00:08 And to give you some anatomical landmarks, so that when we get into the pathology of the eye, you'll be able to understand what's going on, not only from a kind of a structural point of view, but also from a pathologic and cellular point of view. 00:25 Again, I want to acknowledge the hard work and efforts of Dr. José Mata who made all of this possible. 00:31 We're going to look very briefly again, at the innervation of the ocular muscles, we will spend an entire session just talking about how the eye moves, and the various cranial nerve palsies that affect eye movement. 00:46 It's going to be kind of creative redundancy, you'll see it a couple different times. 00:50 But again, we're going to kind of review it very briefly here. 00:54 So, cranial nerve III , innervates a whole bunch of muscles, it's the superior rectus, the inferior rectus, the inferior oblique, and the medial rectus. 01:07 And if cranial nerve III, or any of its outputs are defective, when a patient is staring straight ahead, the net impact will be that there's no input bringing eye back to the middle of the vision, it's going to be pulled down and out largely through the effects on the superior rectus. 01:31 So that's going to be a dominant effect. 01:32 And the eye will look like a lazy eye going down to - down and out because of the residual superior oblique effects. 01:42 If we, on the other hand, hit or nick or destroyed the trochlear nucleus, the trochlear nerve, that's going to be Cranial Nerve number IV, it's going to be supplying the superior oblique. 01:55 So now we cannot pull the eye down and out. 01:58 We really only see that mostly when we try to have the eye look inwards. 02:04 So, the cranial nerve IV palsy, the patient is looking off to the side. 02:09 And their right eye should have the actual iris and pupil down more midline in the mid palpebral fissure, just like the left eye is. 02:21 That right eye however because it cannot be pulled down and out by the trochlear is in the superior oblique, means that it ends up looking up. 02:31 Okay, that's that palsy. 02:34 And then, we can have a cranial nerve VI palsy, cranial nerve VI is going to be innervating the lateral rectus which is going to be important for making the eye look sideways. 02:43 So, when you're looking straight ahead that eye will not be able to pull to the outside and so the cranial nerve palsy is reflected as kind of looking a little bit cross-eyed with just one eye. 02:57 Again, until you play with this a little bit and think about it a lot it can be a little bit confusing. 03:04 We will return, we will have a session that's almost exclusively all about eye movement, but just a brief kind of creative redundancy.
About the Lecture
The lecture Innervation of the Ocular Muscles – Anatomy Review by Richard Mitchell, MD, PhD is from the course Introduction to Ophthalmology.
Included Quiz Questions
What cranial nerves innervate the ocular muscles?
- Cranial nerves III, IV, and VI
- Cranial nerves IV, V, and VI
- Cranial nerves VI, VII, and VIII
- Cranial nerves VII, IX, and X
- Cranial nerves I, II, and V
What occurs as a result of pathology in the nerves supplying the ocular muscles?
- The movements of the eyeball are affected.
- There is profuse tearing from the eye.
- The eye becomes swollen and red.
- There is a purulent discharge from the eye.
- The eye appears normal.
Author of lecture Innervation of the Ocular Muscles – Anatomy Review

Richard Mitchell, MD, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
