Playlist
Show Playlist
Hide Playlist
Infertility

-
Slides Assisted Reproductive Technology and Infertility.pdf
-
Download Lecture Overview
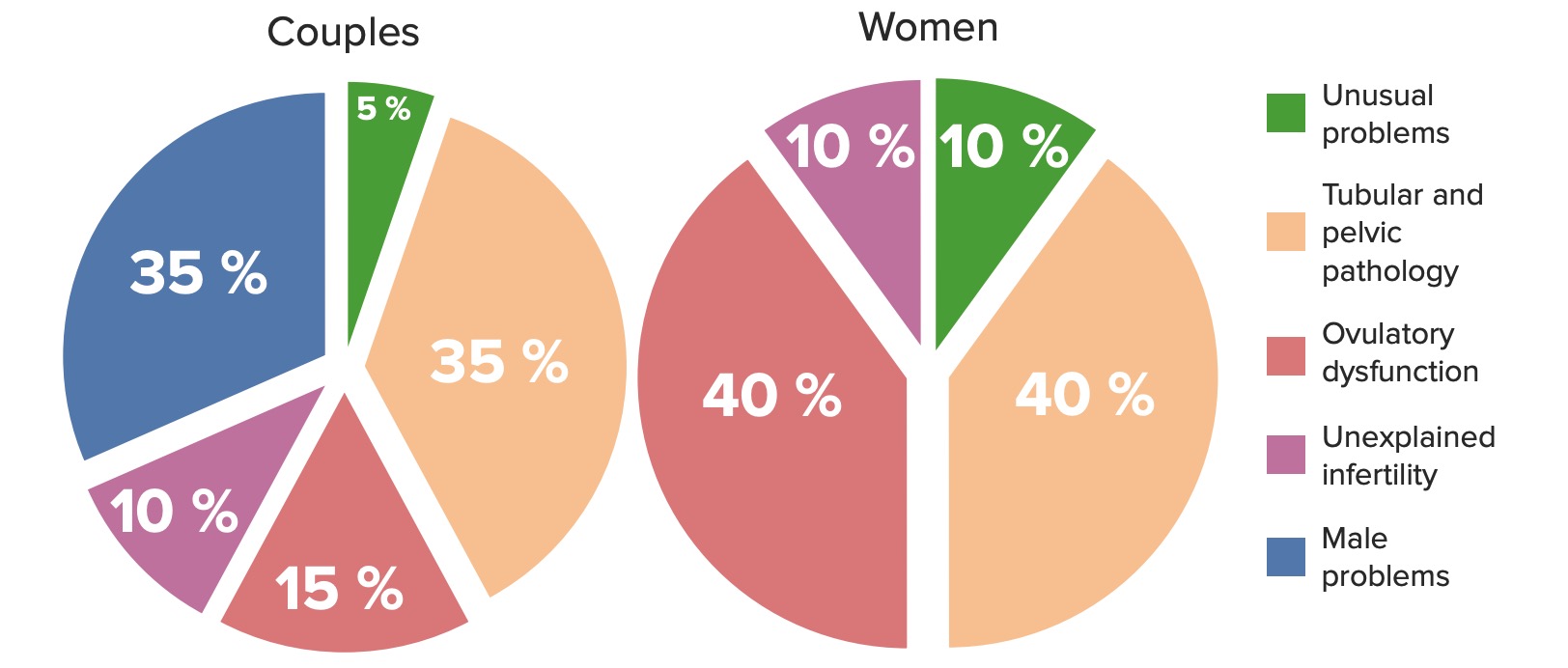
00:00 Hello. This lecture is about assisted reproductive technology in infertility. I doubt you'll have a lot of questions on your USMLE. This is more for your information as you prepare to go to your GYN rotation. Let's go over some definitions. Infertility is 1 year of unprotected intercourse without conception. Usually, this is timed intercourse where people are trying to become pregnant. 00:28 Fecundability is the probability a cycle will result in a pregnancy. While fecundity is the probability that 1 cycle will result in a live birth. Let's review some of the causes of infertility. Unusual problems are very rare while tubal factor infertility and pelvic pathology make up a large percentage in both the woman and the couple. Ovulatory dysfunction is another cause of infertility. 00:58 Unexplained infertility essentially means all their testing is normal yet they still can't conceive. 01:05 Lastly, male problems make up a large percentage of issues within a couple. I want to review with you now a semen analysis. It's important to note the normal volume is 1.5 mL, the pH should be greater than 7.2, the concentration should be 15 million per mL, and the other most important factor among all these factors is motility, it should be greater than 40% and most important factor among all these factors is motility, it should be greater than 40% and the normal forms should be 4%. Let's now talk about ovulatory dysfunction. You may recall this graph from the normal menstrual cycle. We have FSH that increases that actually recruits follicles, the dominant follicle is selected and the LH surge causes that follicle to undergo maturation and re-enter myosis. Once a follicle is ovulated, you see a surge in estradiol near the time of ovulation and then again in the luteal phase. The luteal phase is named so because of the corpus luteum. The corpus luteum primarily functions to make progesterone. This is high yield and is asked over and over again on the USMLE. Let's now review ovulatory dysfunction. 02:26 Remember, this is a large cause of infertility in the US. You can see this ovary here may be familiar. Have you watched the PCOS lecture? Well if you have, you would recall that this ovary looks like pearls on a string. This is a very common presentation of women with PCOS on ultrasound; however, very young women may have a very similar ultrasound and not have any pathology. This patient has a good prognosis for becoming pregnant. Let's talk about tubal factor infertility. 03:05 Remember in our STI lecture we talked about Chlamydia and PID. Chlamydia and PID can destroy your tubes and here we have a picture of an HSG or hysterosalpingogram of a normal woman. Next to that, we have another picture of a woman with hydrosalphinges. Essentially, her tubes have been dilated with fluid that is actually toxic to an embryo. This patient has had a bout with pelvic tuberculosis. This is actually very uncommon in the US but tubal surgery could also look very similar. Also, any adhesions in the pelvis can also block the tubes causing there to be no fill and spill of dye on upon an HSG. There are treatment options for women based on the type of infertility that they suffer from. The question is "Do they have sperm?", "Do they have access to sperm?", "Do they ovulate?", "Do they have normal tubes for fertilization to occur?" If they do have normal tubes, we can actually cause ovulation induction if they're anovulatory, or we can do ovulation induction to increase the risk of superovulation or increasing the number of eggs that they actually release. We can also increase their odds by doing intrauterine insemination. That means, we put sperm into the uterus to increase the changes of sperm reaching the tube. We also can do IVF or in vitro fertilization. Traditionally, before IVF was effective we use zygote intrafallopian tube transfer or Gamete intrafallopian tube transfer. Those are no longer used but you may read about them. If male factor is a problem, we do intracytoplasmic sperm injection. That is we take 1 solitary sperm and inject it to an egg causing it to become fertilized. If you don't have access to sperm or you're anovulatory because you have hypergonadotropic hypogonadism, then we can use donor gametes. That means someone else donates their sperm or an egg. If the intended mother does not have a uterus or has a medical condition which will cause her not to become pregnant, then we can use gestational carriers. This is not allowed in some countries but is legal in the US and the laws vary by state. Finally, we also offer adoption to couples who are infertile. Sometimes this is a better method as pregnancy can be very hazardous for some patients including Turner syndrome patients. I now like to bring your attention to controlled ovarian hyperstimulation. We do this often in anovulatory woman. That is, woman who do not release an egg with ovulation on a consistent basis. We traditionally, for PCOS, used to treat women with clomiphene citrate. 06:16 This is a selective estrogen receptor modulator and has a 10% chance of twinning or having twins. 06:24 It requires an intact HPO axis and again it was the first line for PCOS. It does have the side effect of hot flashes. We now use something different. We use letrozole. Letrozole is an aromatase inhibitor and it prevents androgens from being converted to estrogens. This is an off-label use but now has become first line choice in women who experience anovulation. The pregnancy rates compared to clomiphene are 27.5 versus 19.5%. it improves monofollicular recruitment and therefore decreases twinning. There are side effects but they are less so than the ones with clomiphene citrate. You sometimes can experience nausea and dizziness. Another option for women who are anovulatory for different reasons are gonadotropins. Remember, gonadotropins are organically made from the anterior pituitary. Women who do not have a normal HPO axis such as women who have Kallmann syndrome, they do not secrete FSH and LH and therefore they can be treated with injectable gonadotropins. These medications are also used in IVF or in vitro fertilization to induce superovulation. The average yield is 10 to 12 eggs at the time of retrieval. These medications carry a multiple rate of 20 to 30%. That means if you take this there's a 20 to 30% chance you'll have twins, triplets, or even more. This is very dangerous and has long-term consequences for the patient, the child, and society. These patients must be monitored and have a tailored therapeutic regimen by reproductive endocrinologist or infertility specialist who is typically worth certified. Let's now talk about the HPO axis. Remember, the environment puts input into the central nervous system. The central nervous system speaks to the hypothalamus through neurotransmitters and GnRH is made by the hypothalamus which goes to the anterior pituitary to make FSH and LH. These FSH and LH have receptors in the ovary and the ovary produces hormones that influence the uterus. These hormones are estrogen and progesterone, a normal HPO axis results in a menstrual period. We use this axis to actually gain control and cause superovulation and to perform IVF. It's important to remember this as you'll be tested on this over and over again.
About the Lecture
The lecture Infertility by Lynae Brayboy, MD is from the course Reproductive Endocrinology. It contains the following chapters:
- Infertility
- Treatment Options
- Controlled Ovarian Hyperstimulation
Included Quiz Questions
What is the definition of infertility?
- The inability of a couple to conceive after 12 months of regular intercourse without the use of contraception
- The inability to achieve a pregnancy in one menstrual cycle
- The inability to achieve after one menstrual cycle
- The inability to achieve pregnancy as a result of a procedure—such as tubal ligation, hysterectomy, or vasectomy
- Sperm concentration of less than 15 million/ml
Which of the following values is abnormal in a semen analysis test?
- Sperm concentration = 8 million/mL
- Percent motility = 50%
- pH = 7.3
- Volume = 2.5 ml
- Normal morphology = 6%
Which of the following is the best option to assess a patient with suspected tubal infertility?
- Hysterosalpingogram
- Measure FSH and LH serum levels
- Measure TSH and hCG serum levels
- Laparoscopy
- Pelvic X-ray
Which of the following statements regarding ovulation induction is correct?
- Letrozole is the first-line therapy for ovulation induction in females with polycystic ovary syndrome.
- Clomiphene citrate induces ovulation by inhibiting estrogen production, leading to stimulation of follicle-stimulating hormone release.
- Clomiphene citrate is used for ovulation induction in hypothalamic-pituitary-gonadal axis dysfunction.
- Letrozole is associated with the highest risk of twins among controlled ovarian hyperstimulation therapy.
- Injectable gonadotropins can be useful in treating PCOS.
Which of the following hormonal changes is expected during the luteal phase of the menstrual cycle?
- Increased progesterone
- Increased LH
- Increased FSH
- Decreased B-HCG
- Decreased estrogen
Author of lecture Infertility

Lynae Brayboy, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
