Playlist
Show Playlist
Hide Playlist
Hyperthyroidism: Examination, Symptoms, Diagnosis & Treatment of Thyrotoxicosis


-
Emergency Medicine Bord Thyroid Emergencies.pdf
-
Download Lecture Overview
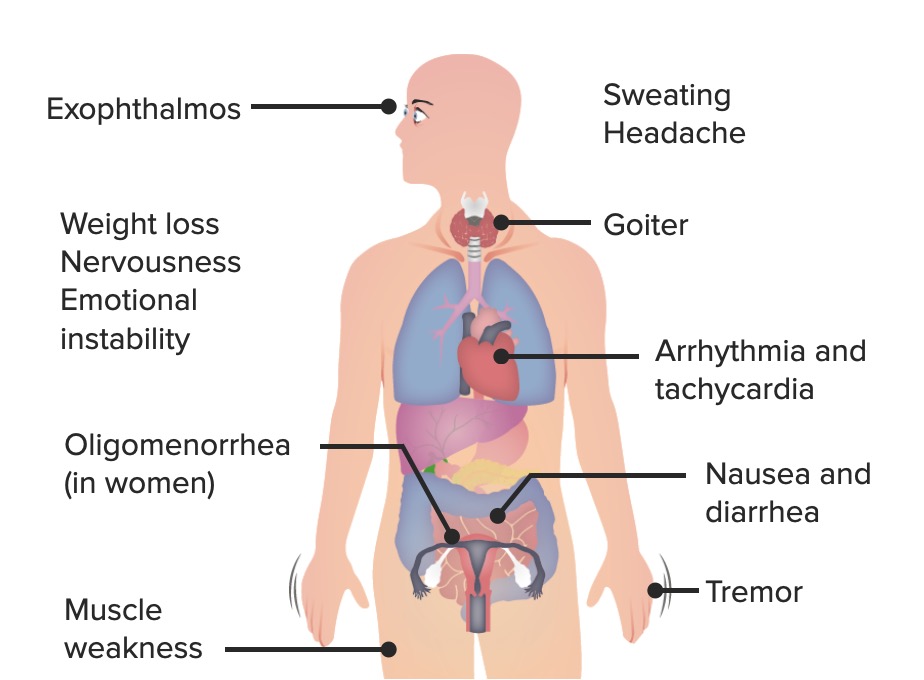
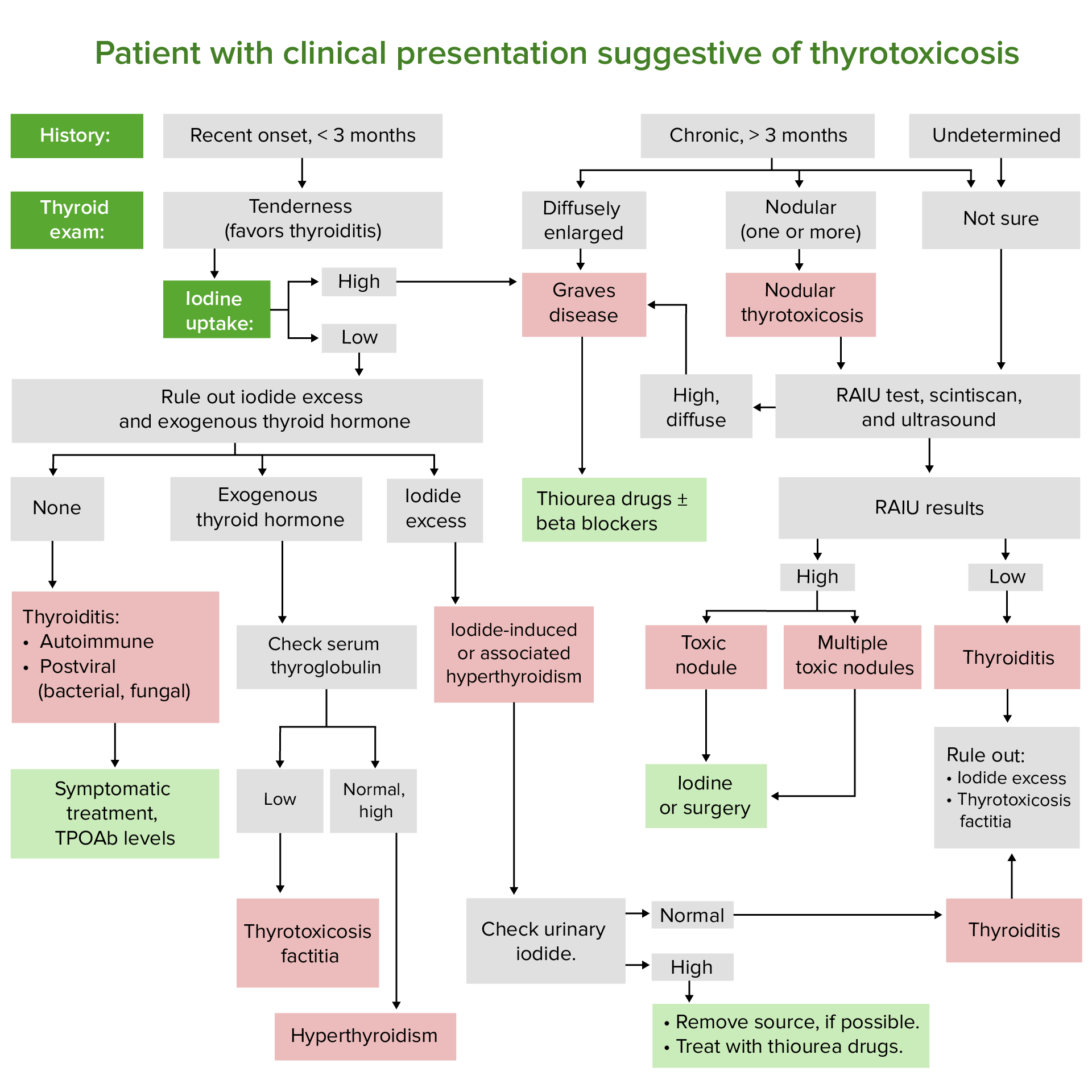
00:01 Now, what are the causes of hyperthyroidism? So Graves' disease is one of the most common causes, toxic multinodular goiter, and then thyroiditis. 00:13 So Graves' is the most common cause for hyperthyroidism. 00:17 It's typically in middle-aged women and it’s due to auto-antibodies which bond to the TSH receptor leading to increased thyroid hormone production. 00:28 Now, there’s the genetic predisposition here. 00:30 So if a family member has it, a first degree relative, then that’s a potential indication or a risk factor for another person getting it. 00:39 Toxic multinodular goiter is due to multiple, autonomously functioning nodules. 00:45 So these are different nodules in the thyroid gland of thyroid tissue. 00:49 And because these are autonomously functioning, they're not talking to each other. 00:53 So that can lead to increased thyroid hormone production. 00:57 This is classically in women greater than 50 years of age. 01:02 And then thyroiditis is due to inflammation of the thyroid gland. 01:05 This picture here is a very dramatic and obvious picture as to what's happening. 01:10 But you can have different causes for thyroiditis. 01:13 You can have suppurative thyroiditis, postpartum thyroiditis, subacute, which means that it takes a longer time to develop. 01:21 Drug-induced thyroiditis which the most classic cause of that being amiodarone. 01:26 And then factitious thyroiditis for patients who ingest excess thyroid hormone than what they’re supposed to or take thyroid hormone when they’re not supposed to. 01:35 That can cause inflammation of the thyroid gland. 01:39 You know, symptoms may be vague, especially in the elderly. 01:42 So old people may not present with the classic symptoms, that you’re expecting them to for hyperthyroidism. 01:50 What are the classic historical elements here? So again, we're focusing on things that are gonna increase the basal metabolic rate. 01:58 So you’re gonna have weight loss. 02:00 So people are gonna be trying to gain weight, or eat their normal diet, but their gonna be losing weight. 02:05 Heat intolerance is gonna be the person who's in the room, who’s always like, "Is it hot in here?" They may feel anxious. 02:13 Cardiovascular symptoms like palpitations, dyspnea on exertion, possibly chest pain and they may actually be in an arrhythmia. 02:21 They may go into atrial fibrillation, related to elevated thyroid hormone. 02:28 They may have dysphagia due to an enlarged gland. 02:31 So based on the location of the gland that it’s in the anterior portion of the neck, when someone swallows, if that gland is large enough, it may cause discomfort with swallowing. 02:42 Patients may have nausea, vomiting, and diarrhea. 02:46 They may have tremors and proximal muscle weakness. 02:50 And they may have eye findings. 02:52 So ophthalmic stuff. 02:53 They may have diplopia, they might feel like something is in their eye and on examination, you might see signs of sympathetic stimulation. 03:03 So the vital signs the patient might be tachycardic. 03:05 They may have a fever and increased pulse pressure and within that tachycardia, they may have atrial fibrillation. 03:13 So their heart beat maybe irregular. 03:15 They might have some evidence of heart failure due to the increased stress that’s placed on the heart. 03:21 The skin is classically warm and flushed, and red. 03:26 Thinning of the hair is something that a patient might report to you or might be seen. 03:31 They might have hyperpigmentation of the pretibial area. 03:35 They might have plaques, nodules, swelling in that area. 03:39 And then lastly, you’re gonna wanna examine their thyroid. 03:42 The thyroid is classically examined by standing behind a person and feeling the thyroid gland in their neck, and having them swallow. 03:50 The thyroid gland will move up and down, as a patient swallows. 04:00 The patient may also have a palpable thrill over their thyroid gland and you may also be able to feel nodules. 04:08 The eye findings are a classic finding for Graves' disease. 04:13 It's due to increased sympathetic stimulation and what happens here is the increased stimulation leads to widening of the palpebral fissures. 04:20 This patient has a characteristic stare. 04:23 Where the eyes are almost bulging out of their head. 04:26 This is known as exophthalmos. 04:29 This is very classic for patients with hyperthyroidism. 04:34 Patients have hyperthyroidism for the most part, those patients are stable and can be treated as an outpatient and diagnosed. 04:43 We are very concerned about patients who are in thyroid storm. 04:47 So thyroid storm is a life threatening form of severe thyrotoxicosis. 04:51 And it actually has 100% mortality if untreated. 04:56 You know, it’s due to either untreated or under-treated thyrotoxicosis, so untreated or undertreated hyperthyroidism. 05:04 And then sometimes, there’s an acute precipitant. 05:07 Did the patient have surgery on her thyroid gland? Has been trauma or any infection? Do they have a pulmonary embolus can be associated or precipitant of this. 05:18 Patients will have fever, very high fever classically. 05:23 So to 104 to 106 Fahrenheit or 40 to 41 degrees Celsius. 05:28 They may have a clinical picture similar to thyrotoxicosis. 05:31 So they may be tachycardic, hypotensive, they may be in atrial fibrillation. 05:37 You might see that characteristic eye findings that you see with hyperthyroidism. 05:41 Patients will have altered mental status. 05:45 They'll be confused, their mental status may be depressed, and then ultimately, cardiovascular collapse. 05:53 Now, you need to suspect this diagnosis based on clinical picture. 05:56 On labs, the patient will have a low TSH. 06:00 They may be very depressed or might be undetectable. 06:03 You wanna check free T4 and T3 levels. 06:07 It's important to remember that only the free T4 and T3 are biologically active. 06:13 Patients may also have elevated blood sugar due to catecholamine responses. 06:18 You can get an ultrasound of the thyroid gland to look for multiple nodules, you can get the ultrasound to look for increased swelling or increased blood flow to that area as well. 06:29 And then an EKG to look for any kind of arrhythmia, to look for atrial fibrillation, to look for a source for the patient palpitations, and to see if there is any EKG changes. 06:42 Now, the differential diagnosis here can be quite broad. 06:44 Some of these symptoms that the patients are presenting with for just plain old hyperthyroid can be a little bit non-specific. 06:52 As we get into thyroid storm, they get a little bit more specific as time goes on with the high fever and the other cardiovascular findings. 07:00 But potentially, it could be anxiety that the patient is experiencing. 07:04 The patient could have anti-cholinergic toxicity, neuroleptic malignant syndrome or serotonin syndrome. 07:13 So patients with a fever, with tachycardia, you start thinking about NMS, and you start thinking about serotonin syndrome. 07:20 You know, when we realized that someone is having thyrotoxicosis and possible thyroid storm, we wanna start out by treating them with support of treatment. 07:30 That essentially means, you wanna give them an antipyretic, you wanna decrease their fever. 07:34 If they're agitated, you wanna give them a benzodiazepine. 07:38 And then you wanna look for the underlying cause. 07:41 You wanna start thinking about why the patient is in this state. 07:45 Then you wanna move on to additional treatment. 07:47 So beta blockade, especially propranolol is recommended. 07:51 What propranolol does is it blocks conversion of T4 to T3 in the periphery. 07:57 You can give this medication orally or IV and it’s also non-selective. 08:00 So it can help with the tremors the patient is experiencing or irritability, that anxiety sensation. 08:07 Then you wanna think about thyroid directed treatment. 08:10 And your goals there are to first of all to decrease hormone production, and then to decrease hormone release, and then to inhibit conversion of T4 to T3, 'cause T3 is your active hormone. 08:23 So reducing thyroid hormone production, how do we do that? There’s two choices. 08:28 There’s methimazole and propylthiouracil or PTU. 08:33 Methimazole is longer acting and PTU has the additional benefit of reducing T4 to T3 conversion. 08:39 So it gives you that extra little bang for your buck. 08:42 You also wanna reduce thyroid hormone release. 08:46 You can do that by using potassium iodine, or a Lugol’s solution. 08:51 You need to give a one hour though after giving methimazole or PTU, because if you give it earlier than that, it won’t necessarily have the effect that you want. 09:00 You also wanna inhibit conversion of T4 to T3 and that can be done by administering steroids. 09:10 For the most part, patients with thyroid storm need to be admitted to an ICU level of care. 09:14 They need a monitor bed if they’re in atrial fibrillation, and they need to get treatment emergently.
About the Lecture
The lecture Hyperthyroidism: Examination, Symptoms, Diagnosis & Treatment of Thyrotoxicosis by Sharon Bord, MD is from the course Endocrine and Electrolyte Emergencies. It contains the following chapters:
- Hyperthyroidism
- Hyperthyroidism Examination
- Hyperthyroidism: Signs and Symptoms
- Hyperthyroidism Diagnosis
- Treatment of Thyrotoxicosis
Included Quiz Questions
What is the most common cause for hyperthyroidism?
- Grave's disease
- Toxic multinodular goiter
- Thyroiditis
- Pituitary tumor
- High iodine diet
Which of the following symptoms is not a classical finding in hyperthyroidism?
- Cold intolerance
- Weight loss
- Anxiety
- Palpitations
- Tremors
What beta blocker is used primarily for the management of thyrotoxicosis?
- Propanolol
- Timolol
- Bisoprolol
- Atenolol
- Carvedilol
Which of the medications used for the thyroid-directed treatment of thyrotoxicosis has an additional benefit of reducing T4 to T3 conversion in peripheral tissue?
- Propylthiouracil
- Methimazole
- Potassium iodide
- Lugol's solution
- Corticosteroids
Author of lecture Hyperthyroidism: Examination, Symptoms, Diagnosis & Treatment of Thyrotoxicosis

Sharon Bord, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
