Playlist
Show Playlist
Hide Playlist
Hyperkalemia: Treatment

-
Slides Potassium Disorders Hypo and Hyperkalemia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
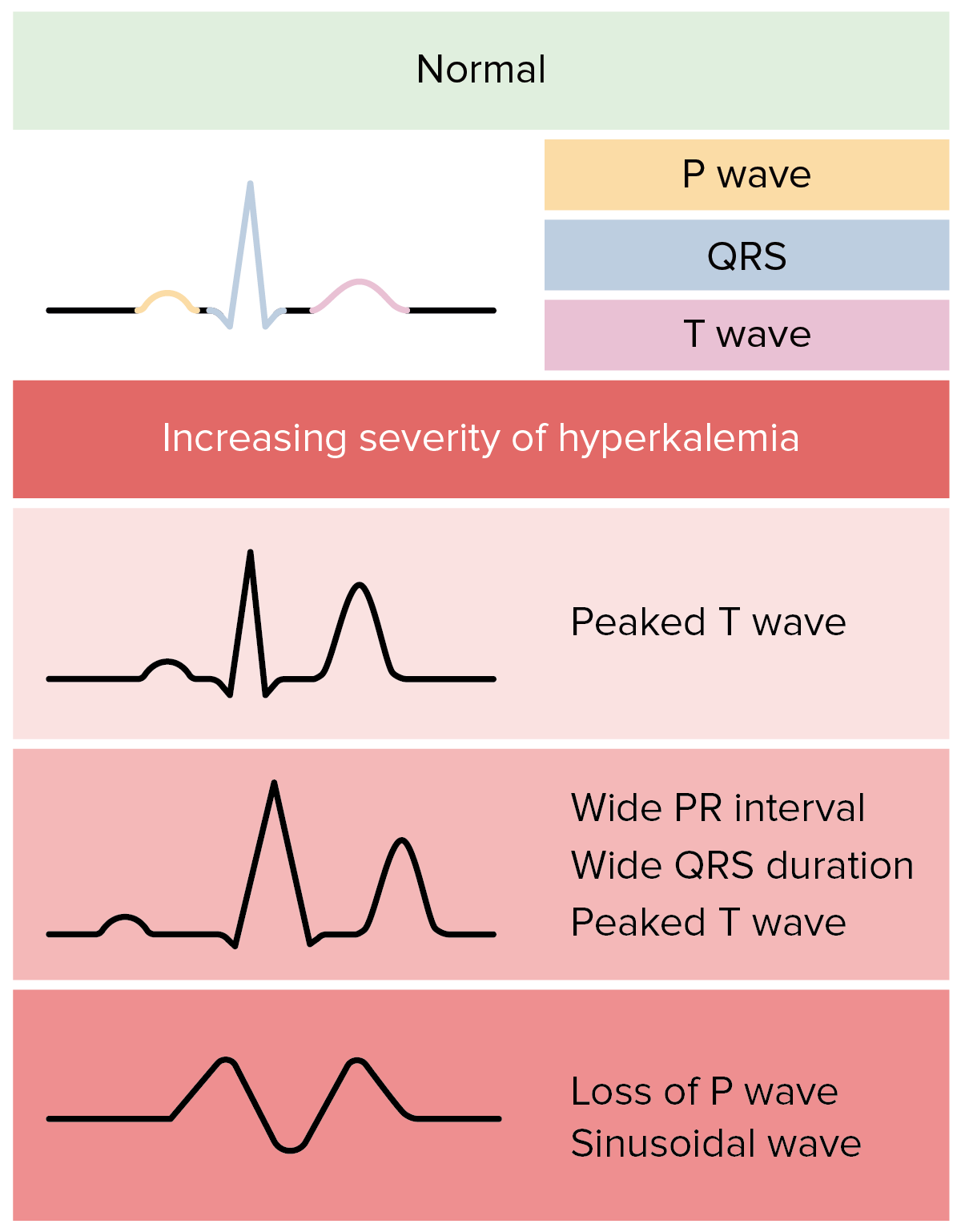
00:01 Once we've determined the etiology of our patients hyperkalemia, it's going to be important to make sure that we can treat them urgently and expeditiously. 00:09 So there's a couple of different things we want to keep in mind. 00:11 Number one. 00:12 We want to potentially antagonize the membrane effects of potassium with calcium if we're worried about cardiac dysrhythmias. 00:18 Number two, we can drive the extracellular potassium into cells. 00:22 And number three, we want to remove that excess potassium from the body. 00:27 So let's talk a little bit more about antagonizing membrane effects of potassium with calcium. 00:31 This is really only going to be reserved for patients who have ECG changes or an acute rise in serum potassium. 00:38 And what I want to tell you is that this does absolutely nothing for removing potassium. 00:42 This is only to protect cardiac myocytes. 00:47 We can use calcium chloride or calcium gluconate, and the mechanism and when we think about in terms of what happens hyperkalemia induces the depolarization of the resting membrane potential, that leads to inactivation of the sodium channels in a decreased membrane excitability. 01:01 So calcium antagonizes this membrane affect. 01:04 The mechanism is not well understood. 01:07 But again, what I want to underscore here is that this is to protect cardiac myocytes. 01:11 It does nothing in efforts to remove excess potassium from the body. 01:16 So the next thing we want to think about in terms of the treatment of hyperkalemia, and what we have in our armamentarium is driving the extracellular potassium into cells. 01:25 So we can do this by using insulin. 01:28 So remember what insulin does it's going to cause uptake of potassium into the cell by stimulating the activity of the sodium-potassium ATPase. 01:35 Now if we're going to give this as a therapy for hyperkalemia, it's going to be important to give it with glucose if our patients are normal glycemic. 01:43 We can also use beta-2 agonists like Albuterol and terbutaline. 01:46 This also stimulates the sodium-potassium ATPase, but it does so through a different mechanism than insulin. 01:53 It actually works through cyclic-AMP. 01:55 Therefore when you use beta agonists along with insulin, it provides a synergistic effect, and it can actually lower potassium by about 1.2 to 1.5 milli equivalents when used together. 02:08 So finally, we're left with our last category, which is removing excess potassium from the body. 02:14 There's a couple of different ways that we can do this. 02:17 Number one is diuretics. 02:18 Remember Loop Diuretics and thiazide diuretics. 02:21 We said by that mechanism of an increase in distal delivery of sodium mediates potassium e-flux into that tubular fluid. 02:28 We can use these therapies in patients who are relatively stable and long-term out patients who have chronic kidney disease. 02:36 Loop Diuretics can also be effective in the short term when combined with saline to maintain that distal delivery of sodium and distal tubular flow, but we rarely do this. 02:46 Another mechanism for potassium removal include using cation exchange resins. 02:52 This includes sodium polystyrene sulfonate otherwise known as kayexalate. 02:56 This is an exchange resin that will take a potassium in the gut and release sodium. 03:01 Now most preparations that are used are prepared using sorbitol. 03:04 That's an osmotic laxative which we'll also add to the mechanism of potassium excretion. 03:10 But what you need to keep in mind is that that's orbital component can actually lead to intestinal necrosis. 03:15 So we have to be very careful about using this medication certainly in our surgical patients who are at highest risk. 03:22 There are other cation exchange resins available too. 03:25 Paitromir, also known as Veltessa. 03:27 This takes up potassium and exchange for calcium in the colon. 03:32 And likely, in the long term this will replace sodium polystyrene sulfonate. 03:36 Another one that's new to the market is zirconium cyclosilicate. 03:40 And this is something that will exchange both sodium and protons for potassium during the intestinal transit. 03:46 Again, this will likely replace sodium polystyrene sulfonate in the long term. 03:51 Finally when we're thinking about potassium removal, probably the most effective way of moving potassium urgently is through dialysis. 04:00 And this is warranted when the prior mechanisms or measures are insufficient to correct the hyperkalemia. 04:06 Or if for example, somebody is expected to have a massive increase in potassium released either because of rhabdomyolysis or tissue breakdown. 04:15 Hemodialysis is going to be the preferred modality because it can remove up to about 25 to 50 Milli equivalents of potassium per hour. 04:23 And it's certainly the treatment of choice in our patients who have end-stage renal disease. 04:28 We also want to think about treating reversible causes. 04:31 So if a patient is on a drug, that's causing hyperkalemia. 04:35 We want to discontinue that drug. 04:36 And finally in our patients who are volume depleted, we want a volume expand them so that we can increase that distal delivery of sodium.
About the Lecture
The lecture Hyperkalemia: Treatment by Amy Sussman, MD is from the course Potassium Disorders: Hypo- and Hyperkalemia.
Included Quiz Questions
What is the role of calcium in the management of hyperkalemia?
- Antagonizes the membrane effects of potassium
- Shifts potassium from the intracellular compartment to the extracellular compartment
- Shifts potassium from the extracellular compartment to the intracellular compartment
- Increases the renal excretion of potassium
- Increases the gastrointestinal excretion of potassium
Which of the following is an adverse effect of sodium polystyrene sulfonate?
- Intestinal necrosis
- Hypoglycemia
- Hyponatremia
- Renal impairment
- Congenital malformations
Author of lecture Hyperkalemia: Treatment

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
