Playlist
Show Playlist
Hide Playlist
Hyperkalemia: Clinical Manifestations and Diagnosis

-
Slides Potassium Disorders Hypo and Hyperkalemia.pdf
-
Reference List Nephrology.pdf
-
Download Lecture Overview
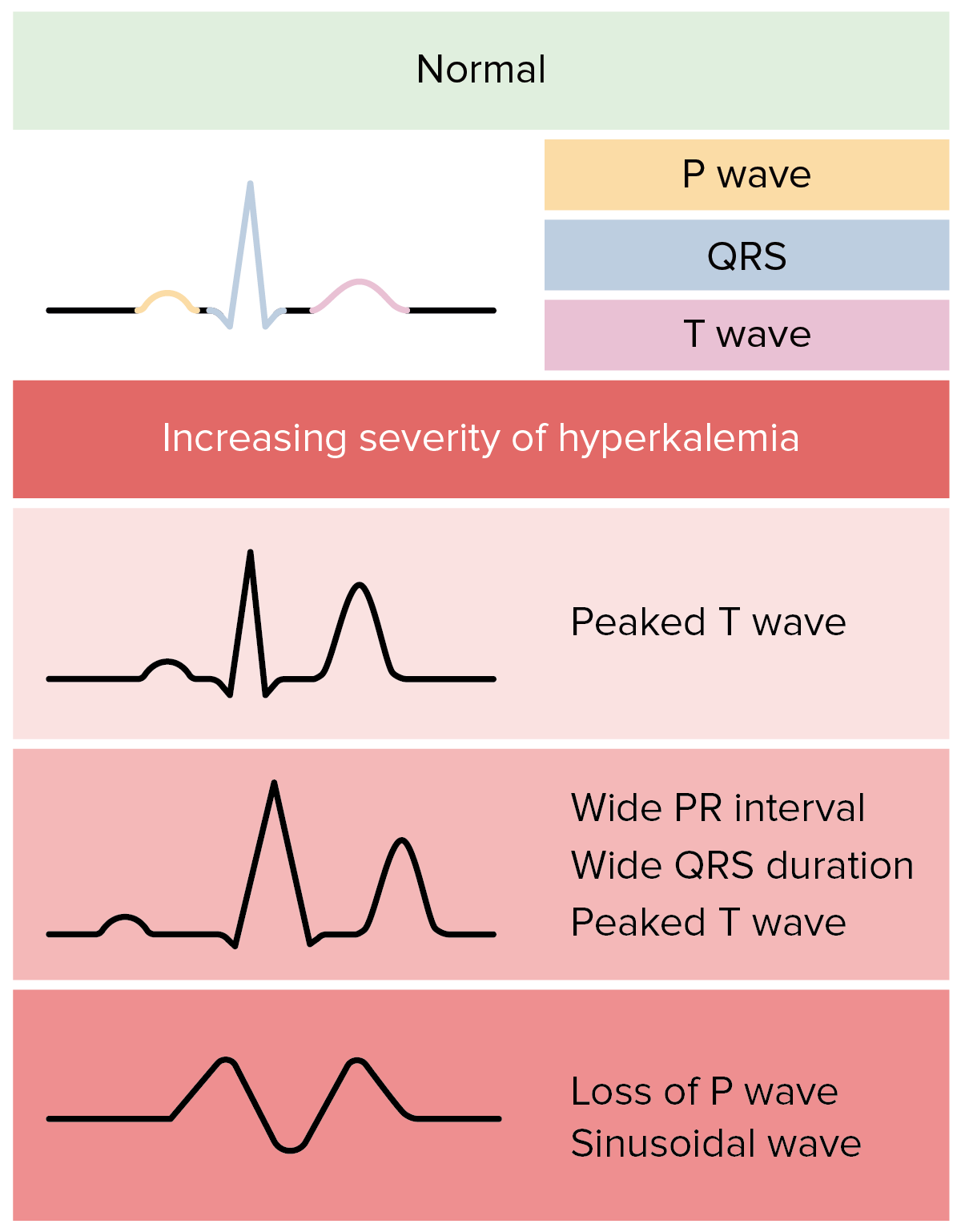
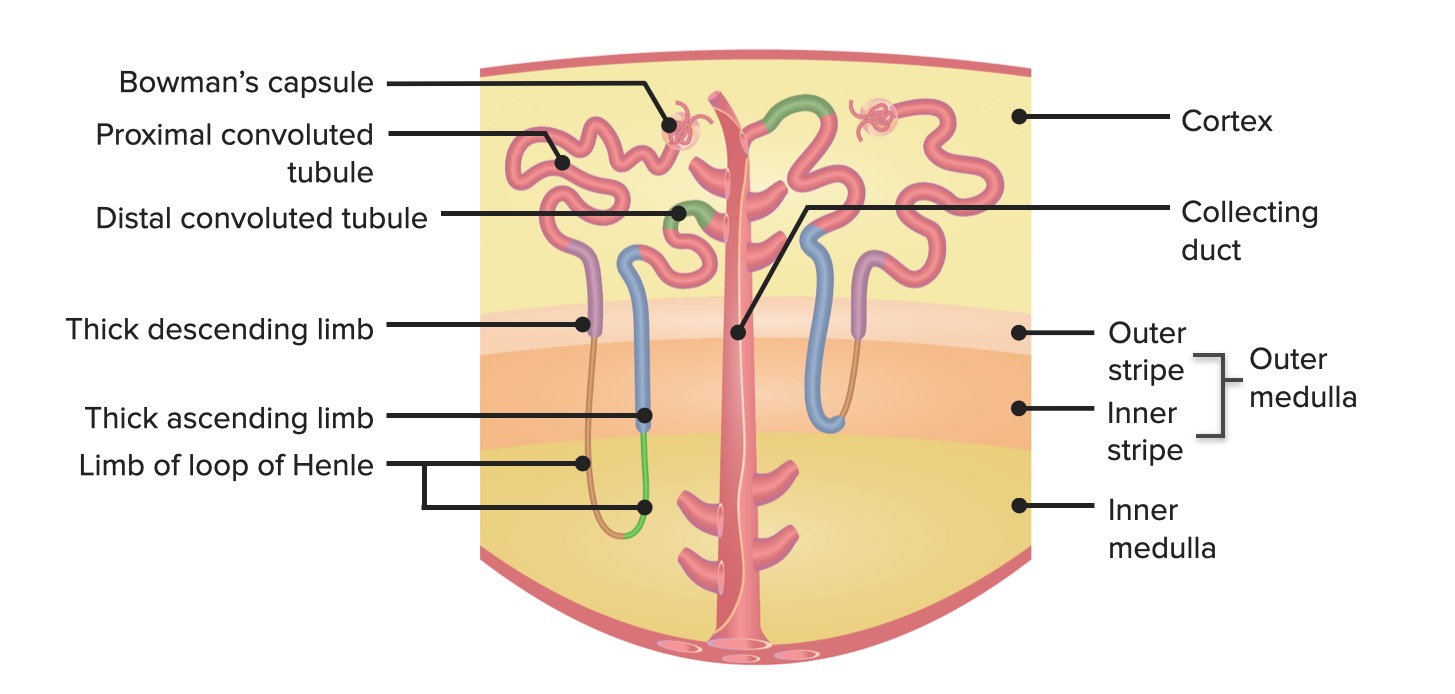
00:01 When a patient presents clinically with hyperkalemia, the way they're going to manifest is they're going to have severe muscle weakness or paralysis and it's often times in ascending weakness that begins with a lower extremities and progresses all the way the trunk upper extremities where they ultimately present with the falccid paralysis. 00:18 They can also have cardiac manifestations. 00:21 So cardiac arrhythmias and EKG abnormalities so they can have bundle branch blocks Advanced atrioventricular blocks sinus bradycardia or sinus arrest. 00:30 A slow idioventricular rhythm or v-tach FIFA relation or asystole essentially everything under the sun from a cardiac standpoint can happen with hyperkalemia. 00:39 So there are some signs on EKG that can also help clue us in to the diagnosis of hyperkalemia. 00:45 What we might see earlier in the course are tall peaked to T-waves and shortening of the QT interval if you look at the top right diagram, you can see an example of peaked T-waves. 00:55 Later in the course, It can actually do generate and you can have prolongation of the PR and QRS interval and widening of the interval and you may actually lose that P wave all together with widening of the QRS where you end up ultimately with the sine wave pattern and that's what's shown on the bottom right. 01:12 If you see an EKG like that you need to move quickly on that patient. 01:18 Once we've determined that our patient has hyperkalemia, it's going to be important to understand and diagnose the underlying cause. 01:25 So will be important to do a good clinical history and physical exam. 01:29 We can measure the plasma potassium in suspected pseudo hyperkalemia. 01:33 We can also look at the plasma renin activity and aldosterone concentration. 01:38 So for example in patients who have a high renin activity, but a low aldosterone we think about things like adrenal insufficiency. 01:47 If our patient has a low renin and a low aldosterone then we think about things like that type for renal tubular acidosis or diabetic nephropathy. 01:56 And finally if our patient has normal to high renin, And a high aldosterone then we think about things that might cause aldosterone resistance that might be tubal interstitial diseases like sickle cell disease or urinary obstruction. 02:08 We can also measure something called the trans tubular potassium gradient and that can help us distinguish between functional hypo aldosterone from other disorders like transcellular shift. 02:19 So what the TTKG is is it's the gradient between the tubular fluid and the plasma potassium and it's going to estimate aldosterone activity by measuring potassium concentration in the tubular fluid at the end of the cortical collecting duct. 02:34 That is really the site of potassium secretion. 02:36 So remember that's where our principal cell is. 02:39 So by looking at the urinary potassium and dividing that by the urine osmolality over the plasma osmolality ultimately over the plasma potassium, we can come up with that trans tubular potassium gradient and a value of less than five is suggestive of hypo aldosterone is meaning that aldosterone is not working appropriately.
About the Lecture
The lecture Hyperkalemia: Clinical Manifestations and Diagnosis by Amy Sussman, MD is from the course Potassium Disorders: Hypo- and Hyperkalemia.
Included Quiz Questions
Which of the following is associated with hyperkalemia?
- Peaked T waves on ECG
- Increased U wave amplitude on ECG
- Muscle weakness that progresses from the upper limb to the lower limb
- Paralysis with increased muscle tone
Which of the following is true regarding the transtubular potassium gradient?
- It is used to assess the degree of aldosterone activity.
- It has a high value in type 4 renal tubular acidosis.
- It is used in cases of suspected pseudohyperkalemia.
- It measures potassium urine concentration at the end of the ascending limb of the loop of Henle.
Author of lecture Hyperkalemia: Clinical Manifestations and Diagnosis

Amy Sussman, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
